Last updated on May 20, 2026
MetLife Form O93 O 2003-2026 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
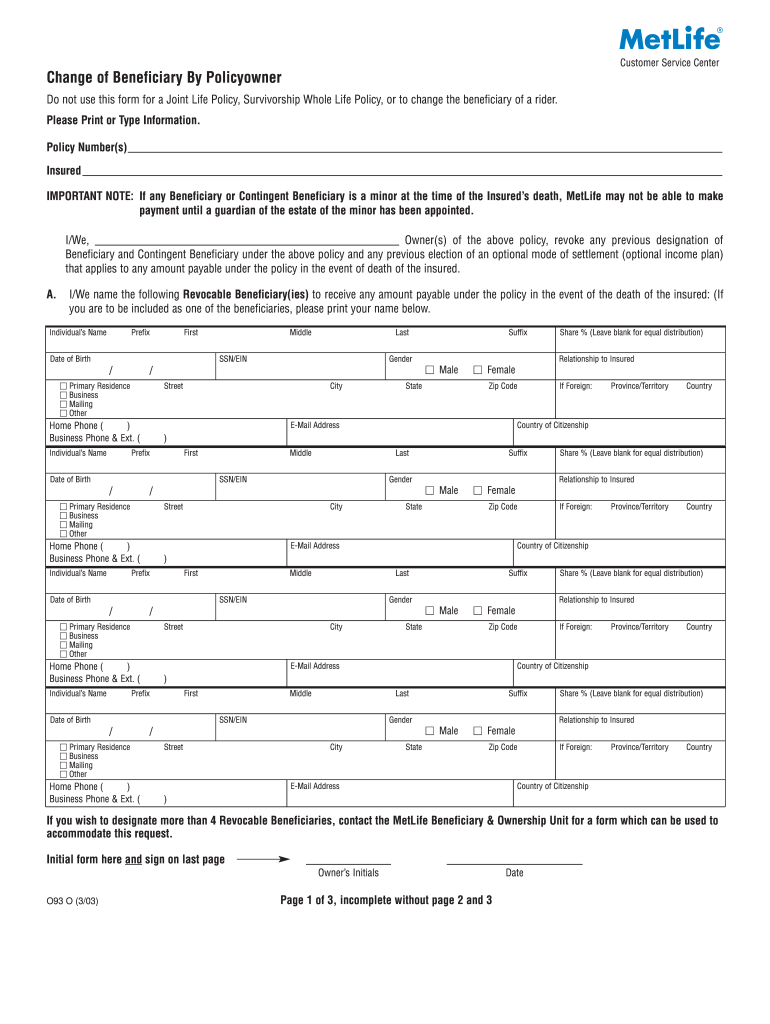
What is MetLife Form O93 O
The Change of Beneficiary Form is a business document used by policyowners to update the beneficiaries of their life insurance policies with MetLife.
pdfFiller scores top ratings on review platforms
Who needs MetLife Form O93 O?
Explore how professionals across industries use pdfFiller.

MetLife Form O93 O is needed by:
-
Policyowners looking to update their beneficiaries
-
Witnesses for signing the change of beneficiary form
-
Insurance agents assisting clients with beneficiary changes
-
Legal professionals handling estate planning
-
Individuals managing life insurance policies
Comprehensive Guide to MetLife Form O93 O
What is the Change of Beneficiary Form?
The Change of Beneficiary Form is a crucial document utilized by policyowners to modify the beneficiaries listed on their life insurance policies. This form is directly relevant for updating beneficiary information with providers like MetLife. It necessitates specific information such as the policy number, the insured’s name, and details about the new beneficiaries, including their names, dates of birth, and relationship to the insured.
Purpose and Benefits of the Change of Beneficiary Form
This form serves essential functions for policyowners and beneficiaries alike. It safeguards the interests of policyowners by ensuring that beneficiary information is current and reduces the likelihood of disputes surrounding life insurance proceeds after the insured has passed away. By regularly updating beneficiaries, policyowners can ensure that their intentions are honored, providing peace of mind.
Who Needs the Change of Beneficiary Form?
Various individuals and circumstances may necessitate the use of this form. Policyowners who have changed their personal circumstances, such as through marriage, divorce, or the death of a previous beneficiary, should consider filling out the Change of Beneficiary Form to reflect these changes accurately. Keeping beneficiary information up-to-date is essential for proper estate planning and ensuring that funds are allocated according to the policyowner’s wishes.
How to Fill Out the Change of Beneficiary Form Online (Step-by-Step)
Filling out the Change of Beneficiary Form online can be straightforward if you follow these steps:
-
Open the form and enter your name, date of birth, and Social Security Number (SSN).
-
Provide the insured's name and policy number, ensuring accuracy.
-
Add the new beneficiaries’ details, including their names and contact information.
-
Specify each beneficiary's relationship to the insured and their date of birth or SSN.
-
Review all entries for completeness.
-
Sign and have the form witnessed by an adult who is not a beneficiary.
Common Errors and How to Avoid Them
When completing the Change of Beneficiary Form, certain errors can occur. Common mistakes include leaving fields incomplete or providing incorrect signatures. Additionally, triple-check all required information before submission to avoid processing delays. Ensuring that all sections are fully and accurately filled out is critical to prevent complications in the future.
How to Sign the Change of Beneficiary Form
Understanding the signing requirements for the Change of Beneficiary Form is essential. Both the policyowner and a witness must sign the form. If submitting online, be familiar with the differences between digital signatures and wet signatures, as these may vary based on submission methods. Following the correct signing protocol guarantees that the form is valid and effectively processed.
Where and How to Submit the Change of Beneficiary Form
Once the Change of Beneficiary Form is completed, it must be submitted following specific guidelines. Policyowners can typically send the form directly to their insurance company or agent. Submission methods may include mailing the form, submitting it in person, or uploading the document online, depending on the provider's capabilities.
Confirmation and Tracking Your Submission
After submitting the Change of Beneficiary Form, it is important to confirm that it has been received. Many insurance providers, including MetLife, offer tracking options for submitted forms. Always follow up to ensure that your changes have been processed and recorded in their systems, providing additional peace of mind.
Security and Compliance When Using the Change of Beneficiary Form
When handling the Change of Beneficiary Form, security is paramount. Using platforms like pdfFiller ensures that your sensitive information is protected. With features such as 256-bit encryption, compliance with HIPAA, and GDPR regulations, users can trust that their data will remain confidential and secure throughout the process.
Unlock Easy Form Completion with pdfFiller
pdfFiller provides a seamless experience for filling out the Change of Beneficiary Form. This platform offers significant benefits, including user-friendly features, robust security measures, and extensive support. The ability to electronically sign and securely store your forms makes pdfFiller an ideal choice for policyowners looking for efficiency and safety when managing their life insurance documentation.
How to fill out the MetLife Form O93 O
-
1.Access pdfFiller and search for 'Change of Beneficiary Form' in the document library.
-
2.Open the form by clicking on its title, which will launch the editing interface of pdfFiller.
-
3.Gather necessary information before starting, including the policy number, insured's name, and required details of new beneficiaries.
-
4.Navigate to the fields, which include checkboxes and blank spaces for entering information, ensuring to follow the instructions provided.
-
5.Fill out the names, dates of birth, SSN/EIN, gender, relationship to the insured, and contact information for each beneficiary.
-
6.Review your form as you progress, double-checking for accurate spelling and correct information.
-
7.Once all fields are complete, make sure to initial and sign the last page of the form as required.
-
8.Finalize your form review, ensuring it contains all three pages and follows any additional instructions.
-
9.Save your changes by clicking on the 'Save' button, or download the filled-out PDF directly to your device.
-
10.Submit the completed form as per instructions provided, either by mailing it to MetLife or following any additional submission guidance.

Who is eligible to use the Change of Beneficiary Form?
Any policyowner of a MetLife life insurance policy is eligible to use the Change of Beneficiary Form to update their beneficiaries.
What information do I need to complete this form?
You will need your policy number, the insured’s name, and detailed information about the new beneficiaries, including their names, dates of birth, SSN/EIN, gender, relationship, and contact details.
How do I submit the Change of Beneficiary Form?
After completing the form, you can submit it by mailing it to MetLife or following any specific submission guidelines provided in the instructions accompanying the form.
Are there any common mistakes to avoid when filling out this form?
Common mistakes include leaving fields blank, misspelling names, or not following the signing requirement set for both the owner and the witness.
What should I do if I need to make changes after completing the form?
If changes are necessary after submitting, contact MetLife directly for guidance on amending your beneficiary designations.
Is notarization required for the Change of Beneficiary Form?
No, notarization is not required for the Change of Beneficiary Form. However, it must be signed by the owner and witnessed by a disinterested adult.
How long does it take for changes to be processed?
Processing times can vary, but typically it takes a few business days for MetLife to update beneficiary information after receiving the completed form.
Related Content
Related Forms

Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.