Last updated on May 20, 2026
Get the free cigna dental claim form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
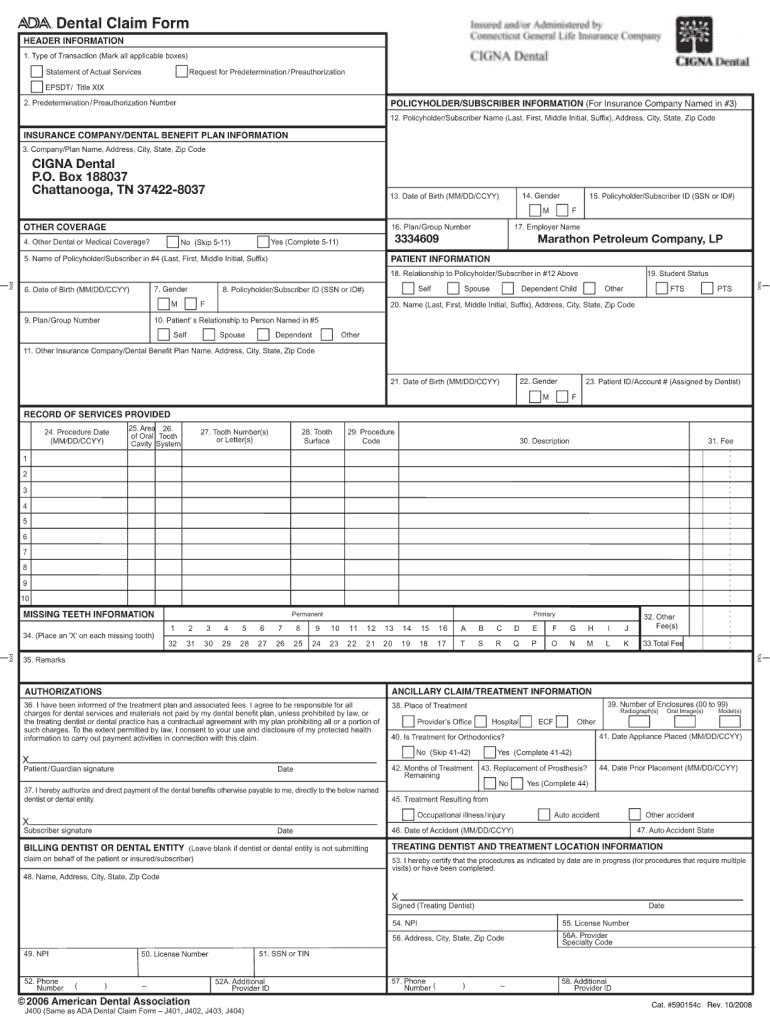
What is cigna dental claim form
The Cigna Dental Claim Form is a document used by policyholders to file claims for dental services covered under their Cigna insurance plan.
pdfFiller scores top ratings on review platforms
can't pull up blank version of pre form used
Fabulous user friendly interface.. Which helps because nobody fills out court papers for anything fun... Normally court=stress. Your help negated that stress greatly.
Who needs cigna dental claim form?
Explore how professionals across industries use pdfFiller.

Cigna dental claim form is needed by:
-
Cigna dental insurance policyholders
-
Dentists submitting claims on behalf of patients
-
Healthcare administrators managing dental claims
-
Individuals seeking reimbursement for dental expenses
-
Financial coordinators in dental clinics
-
Insurance agents supporting clients with claims
Comprehensive Guide to cigna dental claim form
What is the Cigna Dental Claim Form?
The Cigna Dental Claim Form is a crucial document used in the process of dental insurance claims. It allows policyholders to seek reimbursement for dental services they have received. By completing this form accurately, users can ensure they receive timely financial support for their dental treatments.
Purpose and Benefits of the Cigna Dental Claim Form
The Cigna Dental Claim Form is necessary for submitting dental claims efficiently. Utilizing this form provides several benefits, including simplifying the claims process and facilitating faster reimbursements for policyholders. Timely submission of the completed form can help you receive your deserved financial support more quickly.
Who Needs the Cigna Dental Claim Form?
This form is essential for Cigna policyholders and their dependents who seek reimbursement for dental services. Scenarios when the form is typically needed include visits to in-network and out-of-network dental providers, as well as for various dental treatments and procedures.
How to Fill Out the Cigna Dental Claim Form Online
To fill out the Cigna Dental Claim Form online, follow these steps:
-
Access the Cigna Dental Claim Form using pdfFiller.
-
Fill in the necessary fields with accurate information.
-
Utilize the editing tools to review and correct your entries before submission.
Tips for navigating the online form features include using the save option frequently and checking for auto-fill options to save time.
Field-by-Field Instructions for the Cigna Dental Claim Form
Understanding the fields on the Cigna Dental Claim Form is essential for successful completion. Key components include:
-
Patient information: Provide accurate personal details to prevent processing delays.
-
Provider details: Ensure all provider information is correct and complete.
-
Treatment descriptions: Clearly outline the treatments received to avoid confusion.
Common errors to avoid when filling out specific sections include typos in patient data and incomplete treatment descriptions. Double-checking entries can significantly reduce the chances of rejection.
Submission Methods for the Cigna Dental Claim Form
There are several methods available for submitting the completed Cigna Dental Claim Form:
-
Online submission via pdfFiller for immediate processing.
-
Mailing the form to Cigna for traditional processing.
-
Faxing the completed form directly to Cigna.
For ensuring submission accuracy, it is best to verify that all fields are fully completed and to keep a copy of the submission for your records.
Tracking Your Cigna Dental Claim Submission
After submitting your claim, you can track the status by contacting Cigna directly. It is essential to have your claim number on hand for efficient follow-up. Expect timelines for processing to vary, but many claims are reviewed within a standard timeframe.
Common Reasons for Claim Rejections
Claims can be rejected for several reasons, including:
-
Incomplete or inaccurate patient information provided.
-
Insufficient documentation accompanying the claim.
-
Claims submitted outside the allowable time frame.
Providing complete and accurate information is crucial to avoiding issues and enhancing the chances of approval.
Security and Compliance in Handling the Cigna Dental Claim Form
When using the Cigna Dental Claim Form, document security is a top priority. pdfFiller ensures compliance with regulations such as HIPAA and GDPR, safeguarding your personal information during the claim process. Users can confidently complete their forms knowing that their data is treated with the utmost confidentiality.
Ready to Get Started with Your Cigna Dental Claim Form?
Utilize pdfFiller’s tools to fill out your Cigna Dental Claim Form efficiently and securely. Features such as eSigning and easy sharing can help streamline the claims process, making it easier for you to manage your dental claims.
How to fill out the cigna dental claim form
-
1.To access the Cigna Dental Claim Form on pdfFiller, visit the pdfFiller website and search for 'Cigna Dental Claim Form' in the document library.
-
2.Once you find the form, click on it to open the document in the pdfFiller interface, where you can start editing.
-
3.Before filling out the form, gather necessary information, including your Cigna policy number, details of the dental services received, dates of service, and dentist information.
-
4.Use the toolbar in pdfFiller to fill in the required fields, ensuring accuracy and completeness; hover over fields for tooltips if needed.
-
5.As you complete the form, ensure that all sections are filled correctly; double-check for any missing information that might delay your claim.
-
6.After filling in all required information, review the form carefully to confirm all details are correct and that you’ve included the necessary supporting documents.
-
7.Lastly, save your completed form by clicking on the save option in pdfFiller, which allows you to download a copy to your device or submit it directly through the platform.

Who is eligible to use the Cigna Dental Claim Form?
Any individual who has a Cigna dental insurance plan and has received covered services is eligible to use the Cigna Dental Claim Form for filing claims.
What supporting documents are required when submitting the form?
You typically need to include copies of the dental treatment receipts, detailed invoices, and any other relevant documentation relating to the services provided.
How can I submit the Cigna Dental Claim Form?
The Cigna Dental Claim Form can be submitted via mail, fax, or electronically if using a digital platform like pdfFiller, where you can complete and send it directly through the interface.
What common mistakes should I avoid when completing the form?
Common mistakes include missing required fields, providing incorrect patient or provider information, and neglecting to attach necessary supporting documents or signature.
How long does it take to process claims submitted with this form?
Processing times can vary, but most claims submitted through the Cigna Dental Claim Form are typically processed within 15 business days, depending on completeness and documentation.
Is notarization required for the Cigna Dental Claim Form?
No, notarization is not required for the Cigna Dental Claim Form; simply complete the necessary fields and submit as directed.
What should I do if my claim is denied?
If your claim is denied, review the denial notice for reasons cited, and consider reaching out to Cigna customer service for clarification or to appeal the decision.
Related Content
Related Forms





Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.