TX CSHCN TP1 2007 free printable template
Show details
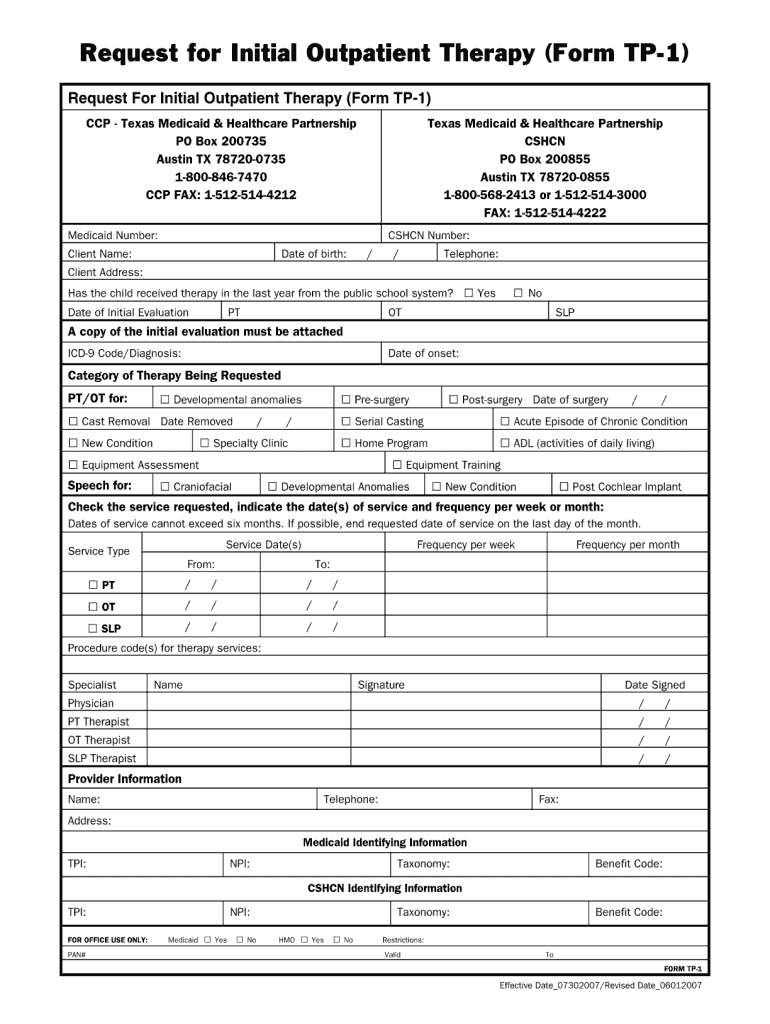
Request for Initial Outpatient Therapy Form TP-1 CCP - Texas Medicaid Healthcare Partnership PO Box 200735 Austin TX 78720-0735 1-800-846-7470 CCP FAX 1-512-514-4212 Medicaid Number Client Name Date of birth / Telephone Client Address Has the child received therapy in the last year from the public school system Date of Initial Evaluation PT OT Yes No ST A copy of the initial evaluation must be attached Date of onset Diagnoses Use ICD-9 diagnosis codes for prior authorization requests...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign TX CSHCN TP1
Edit your TX CSHCN TP1 form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your TX CSHCN TP1 form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit TX CSHCN TP1 online



Use the instructions below to start using our professional PDF editor:
1
Set up an account. If you are a new user, click Start Free Trial and establish a profile.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit TX CSHCN TP1. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Select it in the list of your records. Then, move the cursor to the right toolbar and choose one of the available exporting methods: save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
TX CSHCN TP1 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out TX CSHCN TP1
How to fill out TX CSHCN TP1
01
Begin by gathering all necessary personal information, including your child's name, date of birth, and Medicaid number.
02
Fill out Section A with the child's demographic details.
03
In Section B, provide information about the child's health needs and any medical conditions.
04
Complete Section C with details of the healthcare services the child is currently receiving.
05
If applicable, fill out Section D regarding any special needs or accommodations.
06
Review the entire form for accuracy and completeness.
07
Sign and date the form at the designated area.
Who needs TX CSHCN TP1?
01
Parents or guardians of children with special health care needs.
02
Families applying for financial assistance or support services for children with disabilities.
03
Healthcare providers referring patients to the CSHCN services.
Fill
form
: Try Risk Free
People Also Ask about
What type of insurance requires prior authorization?
Under medical and prescription drug plans, some treatments and medications may need approval from your health insurance carrier before you receive care. Prior authorization is usually required if you need a complex treatment or prescription. Coverage will not happen without it.
What triggers a prior authorization?
The prior authorization process begins when a service prescribed by a patient's physician is not covered by their health insurance plan. Communication between the physician's office and the insurance company is necessary to handle the prior authorization.
How long does it take for Medicaid approval Texas?
Make and document an eligibility decision on an application as soon as all required verification is received. Time frame for eligibility determination: Make an eligibility decision within 45 days on applications from applicants 65 years or older.
What happens if you don't get prior authorization?
No authorization means no payment. Insurers won't pay for procedures if the correct prior authorization isn't received, and most contracts restrict you from billing the patient. PA denials result in lost revenue, declines in provider and patient satisfaction, and delays in patient care.
Does Texas Medicaid require prior authorization?
Except for emergency services, post-stabilization services, and services provided to you during an approved inpatient admission, all services from an out-of-network provider must be prior authorized. Claims for services from out-of-network providers that are not approved before the service is given may be denied.
What is the fax number for Texas Standard Prior Authorization Form?
By fax. Complete the Texas standard prior authorization request form (PDF). Then, fax the form to 1-866-835-9589.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How can I modify TX CSHCN TP1 without leaving Google Drive?
By integrating pdfFiller with Google Docs, you can streamline your document workflows and produce fillable forms that can be stored directly in Google Drive. Using the connection, you will be able to create, change, and eSign documents, including TX CSHCN TP1, all without having to leave Google Drive. Add pdfFiller's features to Google Drive and you'll be able to handle your documents more effectively from any device with an internet connection.
Can I create an eSignature for the TX CSHCN TP1 in Gmail?
You can easily create your eSignature with pdfFiller and then eSign your TX CSHCN TP1 directly from your inbox with the help of pdfFiller’s add-on for Gmail. Please note that you must register for an account in order to save your signatures and signed documents.
How do I edit TX CSHCN TP1 straight from my smartphone?
You can easily do so with pdfFiller's apps for iOS and Android devices, which can be found at the Apple Store and the Google Play Store, respectively. You can use them to fill out PDFs. We have a website where you can get the app, but you can also get it there. When you install the app, log in, and start editing TX CSHCN TP1, you can start right away.
What is TX CSHCN TP1?
TX CSHCN TP1 is a Texas Department of Health form used for reporting information related to children with special health care needs (CSHCN) in the state of Texas.
Who is required to file TX CSHCN TP1?
Providers of health care services for children with special health care needs and certain organizations involved in the care of these children are required to file TX CSHCN TP1.
How to fill out TX CSHCN TP1?
To fill out TX CSHCN TP1, gather the required information about the child and their health care needs, and complete the form by providing accurate and detailed responses as instructed on the form.
What is the purpose of TX CSHCN TP1?
The purpose of TX CSHCN TP1 is to collect data that helps in understanding the health care needs of children with special health care needs in Texas and to enhance service delivery.
What information must be reported on TX CSHCN TP1?
Information that must be reported on TX CSHCN TP1 includes the child's demographics, health care needs, services received, and any special considerations related to their care.
Fill out your TX CSHCN TP1 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
TX CSHCN tp1 is not the form you're looking for?Search for another form here.
Relevant keywords
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
