I understand and agree that the Health Plan may disclose my PHI to a person to whom I have provided my prior permission to release my PHI to in connection with that Person's representation about the Member and their care services. Section B Revocation of Permission To Take the Patient's Biometric Information and Report it to the Commissioner of Insurance, and If Required by the Commissioner of Insurance, to the Health Plan By signing this form, I understand and agree that (I) I understand that a Health Plan may ask me to undergo testing, treatment or examination to obtain or verify my Patient's fingerprint, and that I have consented to this condition; (II) my information may be used by a Health Plan for purposes of billing as well as receiving a medical review, for the purposes of obtaining insurance benefits, and for any other purpose related to my authorization to have my information used by the Health Plan; (III) I am informed of the provisions relating to my data that applies because of my permission to have my information used by the Health Plan; and, (IV) my information may also be used by a third party to report my information to the Commissioner of Insurance and to the Commissioner of Insurance, for their review and for the purposes of the health insurance laws under the Patient Protection and Affordable Care Act. Section C Revocation of Permission By Notifying the Providers and Providers Will Be Discriminated Against By signing this form, I understand and agree that if (v)(i) I have signed this form, an agreement is entered into with the Provider's representative and the Health Plan to obtain information, or (v)(ii) I provide this form to the Provider, the Providers and Health Plan shall not be treated as any different from other Health Plans in any way, and I shall not be the victim of fraud or retaliation. I understand that if I provide this form to the Providers or Health Plan, I am terminating my authorization to have my information used by the Health Plan and the Provider(s) and/or the Health Plan shall be subject to all requirements of the Health Plan.
Get the free release of information
Show details
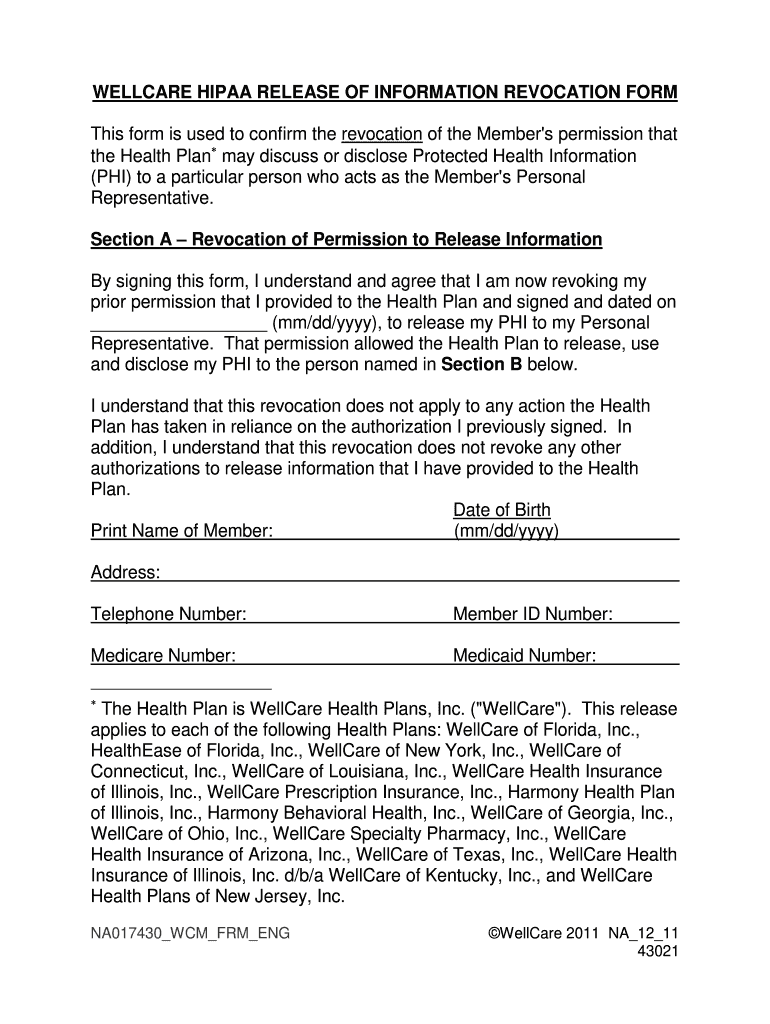
WELL CARE HIPAA RELEASE OF INFORMATION REVOCATION From This form is used to confirm the revocation of the Member's permission that the Health Plan may discuss or disclose Protected Health Information
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign
Edit your release of information form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your release of information form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit release of information online



To use our professional PDF editor, follow these steps:
1
Check your account. If you don't have a profile yet, click Start Free Trial and sign up for one.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit release of information form pdf. Rearrange and rotate pages, add and edit text, and use additional tools. To save changes and return to your Dashboard, click Done. The Documents tab allows you to merge, divide, lock, or unlock files.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
With pdfFiller, it's always easy to work with documents.
Video instructions and help with filling out and completing release of information
Instructions and Help about hippa release form
Hello Dave Guerra real record service how are you thanking you for stopping by today to watch this video today I'm going to talk about the authorization to release health information form it's usually a one-page document I know another medical document you have to fill out, but you know what this is for your own protection because again this lets the hospital the private practice or the clinic know what you need why you need it and who accessed it and who gave it to you the whole nine yards which is a good thing especially when your privacy is at stake, so ideally I'm going to go over the farm from top to bottom and what I'm looking at or what you're going to see is you show up at the medical records department at the clinic or the doctor's office you say hey I need a copy of my medical records well they're going to hand you a form typically like I said one page now they might go into — it just depends on your location there might be your state might require additional notifications that's okay that's strictly up to them so but for the most parts I've encountered one-page documents and usually cram everything in there, but please read the entire document before you fill it out again read the entire document before you start putting your name on that piece of paper now at the top of the form should say the practice the hospital or the clinic that's it has the information next there should be a title and bold letters will say authorization and disclose protected health information authorization to disclose medical records authorization to release protective wealth wise percent protected or health information or medical information again then the next section would be your name we're not necessarily your name the patient's name and that would be like the legal representative you would be the legal representative you would need to put the patient's name down there we go sorry about that, and then you put the patient's full name not like Jake you actually put Jacob not Tony unless that's what it is in his birth certificate NATO how they signed in you would put Anthony otherwise the date of birth now you may be asked for additional information that's okay because again how many Jon semesters in the world and how many John Smith's share the same birthday so again now you might be asked like I said for additional information this would typically be like your address or your social security number maybe like the last four digits or if you have a medical record number that's okay if you don't know problem between you and the medical record clerk you guys you will definitely drill down to get exactly your information the next section will be where you or the legal representative of the patient will authorize the facility the hospital the clinic the private practice and will be written on there or in some cases you have to fill it out yourself that's okay, and you authorize them to disclose the information relating to the above-named individuals' health...
Fill form : Try Risk Free
People Also Ask about release of information
What does a release of information specialist do?
What is a HIPAA release?
What is an authorized release of information?
What does release of information consent mean?
What is a HIPAA authorization for release of information?
What is the purpose of the authorization to release information form?
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is release of information?
Release of information is the process of allowing the sharing or disclosing of an individual's protected health information (PHI) from one party to another, either with or without the individual's consent.
Who is required to file release of information?
Typically, it is the responsibility of healthcare providers, such as hospitals, clinics, and medical practitioners, to file release of information forms when sharing an individual's PHI with another party.
How to fill out release of information?
To fill out a release of information form, you need to include personal details of the individual whose information is being disclosed, specify the recipient(s) of the information, indicate the purpose of the release, and obtain the individual's signature as consent. The form should strictly adhere to legal and privacy requirements.
What is the purpose of release of information?
The purpose of release of information is to provide individuals with control over their own health information. It enables the sharing of PHI between healthcare providers, insurance companies, researchers, and other relevant parties to facilitate proper care coordination, billing, research, and treatment decisions.
What information must be reported on release of information?
A release of information form typically requires the reporting of specific details such as the individual's full name, date of birth, contact information, the type of information being released, the purpose of the release, the recipient(s) of the information, and the duration of the release.
When is the deadline to file release of information in 2023?
The specific deadline to file release of information in 2023 may vary depending on the applicable laws and regulations of the jurisdiction. It is recommended to consult the relevant authorities or legal resources for the accurate filing deadline.
What is the penalty for the late filing of release of information?
The penalties for late filing of release of information can also vary based on jurisdiction and specific circumstances. It is advisable to consult legal resources or government authorities to understand the applicable penalties, which may include fines, sanctions, or other disciplinary actions.
How do I make edits in release of information without leaving Chrome?
release of information form pdf can be edited, filled out, and signed with the pdfFiller Google Chrome Extension. You can open the editor right from a Google search page with just one click. Fillable documents can be done on any web-connected device without leaving Chrome.
Can I create an electronic signature for the hipaa form in Chrome?
Yes. With pdfFiller for Chrome, you can eSign documents and utilize the PDF editor all in one spot. Create a legally enforceable eSignature by sketching, typing, or uploading a handwritten signature image. You may eSign your hippa form in seconds.
How do I fill out the hipaa authorization form pdf form on my smartphone?
Use the pdfFiller mobile app to fill out and sign hipaa form pdf on your phone or tablet. Visit our website to learn more about our mobile apps, how they work, and how to get started.
Fill out your release of information online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Hipaa Form is not the form you're looking for?Search for another form here.
Keywords relevant to hipaa release form pdf
Related to hipaa release of information form




If you believe that this page should be taken down, please follow our DMCA take down process
here
.
