NJ POLST 2012 free printable template
Show details
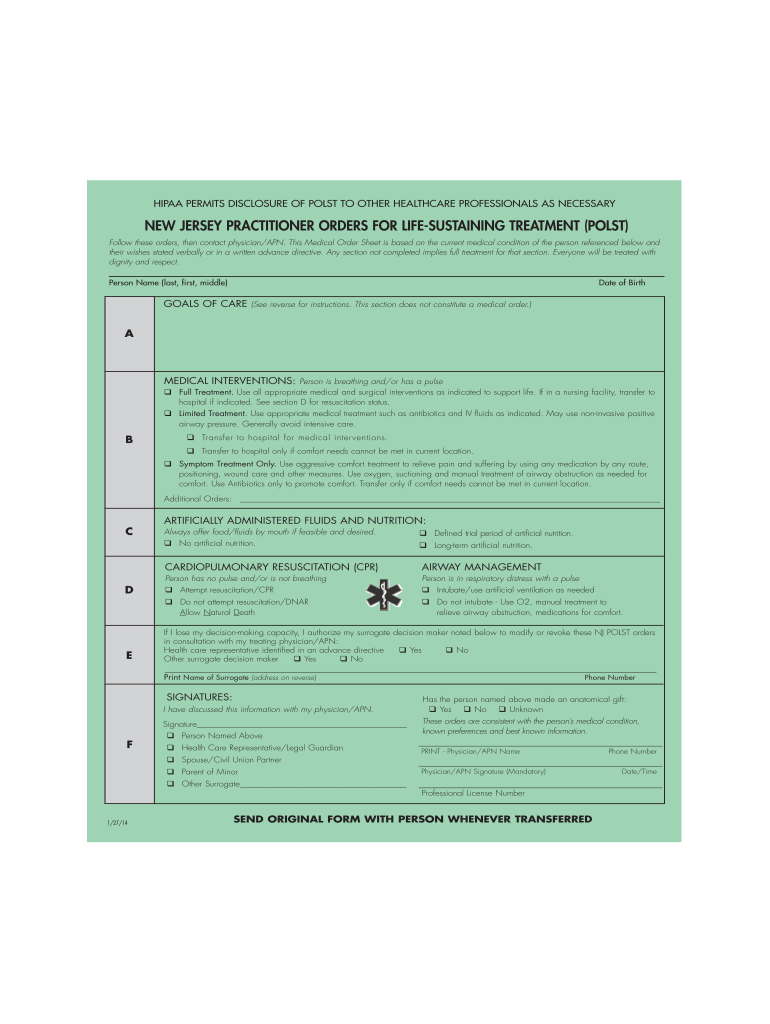
POST GREEN Layout 1 2/26/13 12:18 PM Page 1 HIPAA PERMITS DISCLOSURE OF POST TO OTHER HEALTHCARE PROFESSIONALS AS NECESSARY NEW JERSEY PRACTITIONER ORDERS FOR LIFE-SUSTAINING TREATMENT (POST) Follow
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign
Edit your polst form - new form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your polst form - new form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit polst form - new online



To use our professional PDF editor, follow these steps:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit polst form - new. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Get your file. When you find your file in the docs list, click on its name and choose how you want to save it. To get the PDF, you can save it, send an email with it, or move it to the cloud.
It's easier to work with documents with pdfFiller than you could have ever thought. You can sign up for an account to see for yourself.
NJ POLST Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out polst form - new
How to fill out polst form - new:
01
Begin by gathering all necessary personal information such as name, date of birth, and contact details.
02
Take the time to understand the purpose and significance of each section in the polst form - new.
03
Next, make sure to consult with the individual's healthcare provider or physician to ensure accurate completion of the form.
04
Provide detailed medical history including current diagnoses, medications, and any specific instructions related to treatment preferences.
05
Clearly indicate desired medical interventions in different scenarios such as resuscitation, hospitalization, and use of antibiotics.
06
Complete all required sections, including any optional sections that pertain to the patient's wishes.
07
Review the filled-out form carefully for any errors or omissions before signing and dating it.
08
Discuss the completed polst form - new with healthcare professionals involved in the individual's care to establish a shared understanding of the outlined preferences.
Who needs polst form - new:
01
The polst form - new is recommended for individuals with serious, life-limiting illnesses or advanced stages of chronic conditions.
02
It is crucial for seniors, especially those residing in nursing homes or assisted living facilities, to have a polst form - new in place.
03
Individuals who have previously expressed specific treatment preferences or have requested limited interventions should consider completing a polst form - new.
04
Healthcare providers may also encourage patients with complex medical conditions to have a polst form - new to ensure their wishes are honored during medical emergencies or transitions in care.
Fill form : Try Risk Free
People Also Ask about polst form - new
Can a nurse fill out POLST form?
Can I print a POLST form?
Who can complete a POLST form near new jersey?
Does a NJ POLST need to be signed by a physician?
Is a POLST form mandatory?
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is polst form - new?
The POLST (Physician Orders for Life-Sustaining Treatment) form is a standardized medical document that outlines the patient's preferences regarding life-sustaining treatments and end-of-life care. It is designed to be completed in collaboration with the patient, their healthcare provider, and other relevant individuals, such as family members.
The POLST form is different from an advance directive or living will, as it provides specific medical orders that healthcare providers must follow. It covers various treatment decisions, including the use of cardiopulmonary resuscitation (CPR), artificial ventilation, artificial nutrition and hydration, and other interventions.
The "new" aspect of the POLST form might refer to any recent updates or revisions made to it, as the form may vary slightly depending on the jurisdiction or healthcare system in which it is used. However, the general purpose of the POLST form remains the same: to ensure that patients' treatment preferences are documented and honored by healthcare professionals.
Who is required to file polst form - new?
The POLST (Physician Orders for Life-Sustaining Treatment) form is typically completed by individuals with serious illnesses or advanced medical conditions who wish to outline their preferences for end-of-life medical treatments. This form is not required for everyone but is recommended for individuals who are seriously ill, frail, chronically ill, or have a life-limiting condition. It is often completed in consultation with a healthcare professional, such as a doctor or nurse practitioner. The specific requirements for completing a POLST form may vary by jurisdiction, so it is advisable to consult local regulations and guidelines.
How to fill out polst form - new?
To fill out a POLST (Physician Orders for Life-Sustaining Treatment) form, follow these steps:
1. Obtain the form: Ask your healthcare provider, hospital, or state health department for a copy of the POLST form. You may also find a blank PDF version online, specific to your state.
2. Read the instructions: Before starting, carefully read the instructions on the form. Understand the purpose and significance of each section.
3. Patient information: Include the patient's full name, date of birth, and any other required identifying details at the top of the form.
4. Section A - CPR: Determine the desired level of cardiopulmonary resuscitation (CPR) intervention. Choose one of the following options:
- Attempt CPR: If the patient's heart stops, medical intervention should be initiated.
- Do not attempt CPR: If the patient's heart stops, no CPR attempts should be made.
5. Section B - Medical Interventions: Indicate the patient's preferences regarding medical interventions. Consider the following options and choose what aligns with their wishes:
- Comfort Measures Only: Focus on providing comfort without aggressive treatments or transport to the hospital.
- Limited Additional Interventions: Include specific instructions for interventions like IV fluids, antibiotics, or medical treatments.
- Full Treatment: No limitations or specific instructions. All available interventions are desired, including transfer to the hospital if necessary.
6. Section C - Artificially Administered Fluids and Nutrition: Choose the patient's preferred level of artificial fluids and nutrition:
- Offer Food and Fluids: Provide artificial hydration and nutrition as needed.
- Do Not Offer Food and Fluids: Withhold artificial hydration and nutrition.
7. Section D - Other Instructions: Write any additional specific instructions related to the patient's wishes, such as preferred healthcare facilities, religious considerations, or additional treatment limitations.
8. Signature and date: The patient or their authorized healthcare decision-maker must sign and date the form. If required, ensure that a healthcare professional also signs the form.
9. Distribute copies: Provide copies of the completed POLST form to the patient, their healthcare proxy, and the primary physician. It is also recommended to keep a copy in an easily accessible location, such as the patient's home or wallet.
Remember, while the process of filling out a POLST form is generally standardized, it's important to consult state-specific instructions and guidelines, as some variation exists.
What is the purpose of polst form - new?
The purpose of the POLST (Physician Orders for Life-Sustaining Treatment) form is to ensure that a patient's preferences regarding life-sustaining treatments and interventions are documented and honored in medical settings. The form is typically completed in collaboration with a healthcare professional, and it consists of specific medical orders that guide healthcare providers in delivering appropriate treatment based on the patient's goals and preferences. The form includes instructions for CPR, intubation, medical interventions, and other life-sustaining treatments. It is designed to supplement an advance healthcare directive or living will, providing more detailed and actionable medical orders that are immediately available to healthcare providers in emergencies. The POLST form is especially useful for patients with serious illnesses, advanced frailty, or those near the end of life.
What information must be reported on polst form - new?
The specific information required on a POLST (Physician Orders for Life-Sustaining Treatment) form may vary depending on the region or state. However, some common elements that are typically included in a POLST form are:
1. Patient Identification: Name, date of birth, and contact information of the patient.
2. Medical Orders: Specific medical interventions and treatments that the patient wishes to receive or avoid, including resuscitation, intubation, use of antibiotics, feeding tubes, and artificial hydration.
3. Comfort Measures: Instructions for providing comfort care, pain management, and symptom relief.
4. Life-Sustaining Treatment Preferences: Patient's preferences regarding the use of medical interventions in different situations, such as during cardiac arrest or when suffering from a terminal condition.
5. Signature and Authorization: The form must be signed by the patient or their authorized healthcare decision-maker, and in some cases by a healthcare professional.
6. Healthcare Provider Information: Name, contact information, and signature of the healthcare professional responsible for completing the form.
7. Effective Date: The date when the POLST form becomes effective.
8. Advance Directives: If applicable, any information about the patient's advance directives, such as a living will or durable power of attorney for healthcare.
It is important to note that the specific POLST form requirements can differ between states or regions, so it is crucial to consult the local regulations and guidelines to ensure compliance with all necessary reporting information.
How can I modify polst form - new without leaving Google Drive?
By combining pdfFiller with Google Docs, you can generate fillable forms directly in Google Drive. No need to leave Google Drive to make edits or sign documents, including polst form - new. Use pdfFiller's features in Google Drive to handle documents on any internet-connected device.
How do I execute polst form - new online?
pdfFiller has made filling out and eSigning polst form - new easy. The solution is equipped with a set of features that enable you to edit and rearrange PDF content, add fillable fields, and eSign the document. Start a free trial to explore all the capabilities of pdfFiller, the ultimate document editing solution.
How do I complete polst form - new on an Android device?
Use the pdfFiller Android app to finish your polst form - new and other documents on your Android phone. The app has all the features you need to manage your documents, like editing content, eSigning, annotating, sharing files, and more. At any time, as long as there is an internet connection.
Fill out your polst form - new online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Not the form you were looking for?
Keywords
Related Forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
