Last updated on Apr 4, 2016
Get the free Sample Participant Check Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
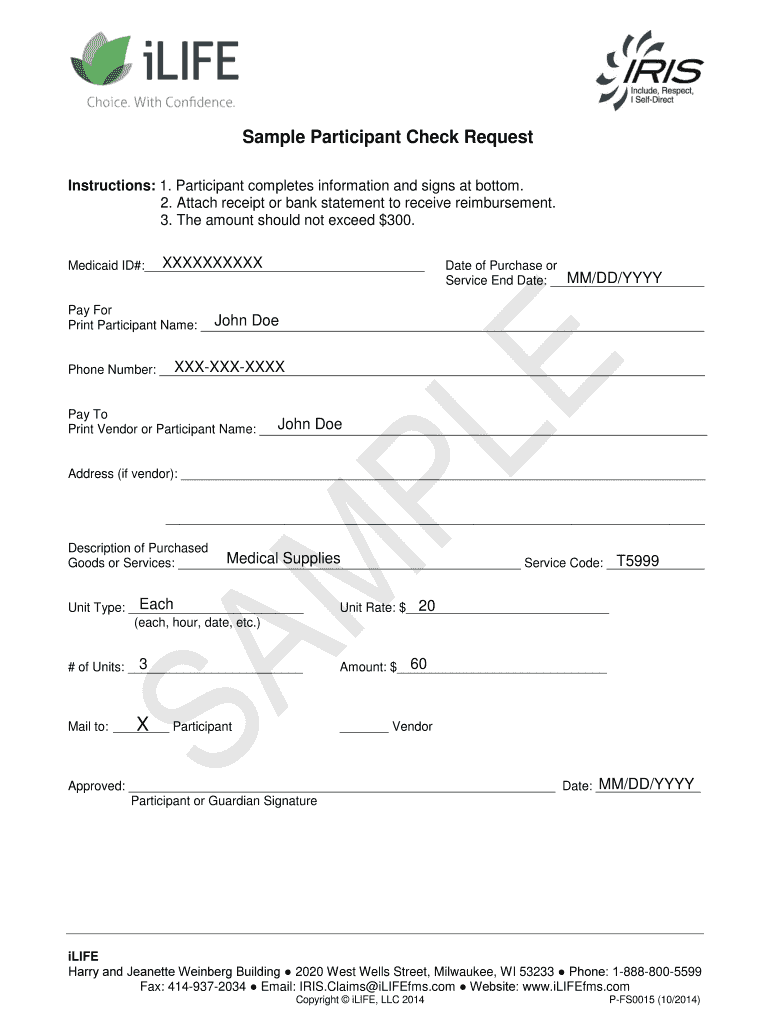
What is Participant Check Request
The Sample Participant Check Request Form is a medical billing document used by participants or their guardians to request reimbursement for medical supplies.
pdfFiller scores top ratings on review platforms
Who needs Participant Check Request?
Explore how professionals across industries use pdfFiller.

Participant Check Request is needed by:
-
Participants seeking reimbursement for medical expenses.
-
Guardians of participants requiring financial compensation for healthcare.
-
Healthcare providers facilitating patient reimbursements.
-
Insurance companies processing Medicaid claims.
-
Billing departments managing medical expense claims.
Comprehensive Guide to Participant Check Request
What is the Sample Participant Check Request Form?
The Sample Participant Check Request Form is designed to facilitate the reimbursement process for medical supplies. Participants or their guardians can use this form to submit requests, ensuring they include essential details such as the Medicaid ID. This form must also meet specific submission requirements to be processed effectively.
Utilizing the participant check request form allows for organized and efficient handling of reimbursement claims. Reimbursements can be processed for medical supplies purchased, making it an essential document for eligible participants.
Purpose and Benefits of Using the Sample Participant Check Request Form
This form streamlines the reimbursement process for participants and their guardians by providing a structured format for requests. The user-friendly design simplifies the submission of claims, eliminating potential confusion or errors.
-
The form accommodates reimbursements up to $300, making it accessible for many participants.
-
Having a clear format aids in improving the speed and accuracy of processing reimbursements.
-
Participants benefit from a straightforward method to recover costs associated with healthcare needs.
Who Needs the Sample Participant Check Request Form?
The Sample Participant Check Request Form is relevant to individuals who are participants in the healthcare program or their guardians. These individuals can complete the form to request reimbursements for specific medical supplies.
-
Eligible medical supplies include items that are necessary for the participant's health and treatment.
-
Residency in Wisconsin is a requirement for eligibility to use this form.
How to Fill Out the Sample Participant Check Request Form Online (Step-by-Step)
Completing the Sample Participant Check Request Form online involves several clear steps that ensure accuracy. Users should follow this structured approach to filling out the form:
-
Start by entering the participant's Medicaid ID in the designated field.
-
Provide detailed information about the medical supplies purchased, including dates and amounts.
-
Include necessary signatures from the participant or guardian where required.
-
Double-check all fields for completeness before submission.
Gathering all required information beforehand enhances the overall efficiency of the process.
Understanding Required Documents and Supporting Materials
Submitting the Sample Participant Check Request Form involves attaching specific supporting documents to validate the reimbursement request. These documents are critical for successful processing.
-
Receipts for the medical supplies purchased must accompany the form.
-
Bank statements may also be required to substantiate the transactions.
-
Maintaining copies of all submitted documents is advisable for personal records.
Submission Methods for the Sample Participant Check Request Form
The completed Sample Participant Check Request Form can be submitted through various methods to accommodate user preferences. Here are the recommended submission methods:
-
Digital submissions can be easily made using the pdfFiller platform, providing convenience and efficiency.
-
For those who prefer physical submissions, printed forms can be mailed to the appropriate address.
-
Tracking submission status is crucial, and users will receive confirmations for their requests.
Common Errors to Avoid when Using the Sample Participant Check Request Form
When filling out the Sample Participant Check Request Form, users should be mindful of frequent errors that can delay reimbursement processing. Here are some common pitfalls to avoid:
-
Missing signatures can lead to rejection of the form—you must ensure they are added.
-
Incorrect Medicaid IDs can result in processing issues; verify accuracy before submission.
-
Using a validation checklist can help confirm that all required fields are completed.
How pdfFiller Enhances Your Experience with the Sample Participant Check Request Form
pdfFiller provides valuable support for users when completing the Sample Participant Check Request Form, enhancing their experience significantly. The platform’s online capabilities make it a top choice for form management.
-
Editing and eSigning features allow users to customize forms easily.
-
Robust security measures, including 256-bit encryption, protect sensitive information during the process.
-
Accessing and filling forms in any browser ensures a seamless user experience.
Final Steps and What Happens After Submitting the Form
After submitting the Sample Participant Check Request Form, users can anticipate several crucial next steps. Understanding the process helps manage expectations.
-
Confirmations are issued once submissions are received, providing peace of mind.
-
Users can track the status of their requests to stay informed about their reimbursements.
-
Potential outcomes include timely reimbursements or requests for additional information.
Start Your Reimbursement Process with pdfFiller Today!
Utilizing pdfFiller for your Sample Participant Check Request Form needs is a proactive choice that simplifies the reimbursement process. The platform's user-friendly features support efficient form completion and submission, ensuring all requirements are met securely.
How to fill out the Participant Check Request
-
1.To access the Sample Participant Check Request Form on pdfFiller, go to the pdfFiller website and use the search function to locate this specific form.
-
2.Once you've found the form, click on it to open it in the interactive editor. Familiarize yourself with the interface to understand where each section is located.
-
3.Before filling out the form, gather necessary information such as the participant’s Medicaid ID, details of the medical supplies purchased, and a copy of your receipt or bank statement.
-
4.Begin filling out the form by clicking on any blank field to input your details. Use the text boxes to enter the participant’s Medicaid ID and all pertinent purchase information.
-
5.Carefully check the boxes that apply to your request, ensuring you include all required details for completeness.
-
6.Review the completed form thoroughly to verify accuracy. Make sure all required fields are filled, and the necessary signature is included at the end of the form.
-
7.Once you are satisfied with the form, save your progress. You can download it directly as a PDF or submit it electronically through the options provided on pdfFiller.

Who is eligible to use the Sample Participant Check Request Form?
Eligible users include participants and guardians who are seeking reimbursement for medical supplies under Medicaid. Ensure you have the participant’s Medicaid ID for processing.
Is there a deadline for submitting the check request form?
While specific deadlines are not detailed in the metadata, it's essential to submit reimbursement requests promptly after medical supply purchases to avoid delays in processing.
What documents need to be submitted with this form?
You must submit a receipt or bank statement along with the Sample Participant Check Request Form to validate your purchase through Medicaid.
How can I submit the completed form?
You can submit the completed form electronically via pdfFiller, download it for mailing, or deliver it directly to your Medicaid provider as required.
What common mistakes should I avoid when filling out the form?
Common mistakes include missing signatures, omitting required identification numbers, and failing to include necessary supporting documents such as receipts.
What is the processing time for this reimbursement request?
Processing times can vary, but it often takes several weeks to process reimbursement requests. Check with your Medicaid provider for more specific timelines.
What if I have questions while filling out the form?
If you encounter issues while completing the form, pdfFiller typically offers support resources. Additionally, consider contacting your healthcare provider for guidance.
Related Forms





Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.