Last updated on Apr 7, 2016
Get the free Patient Referral Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
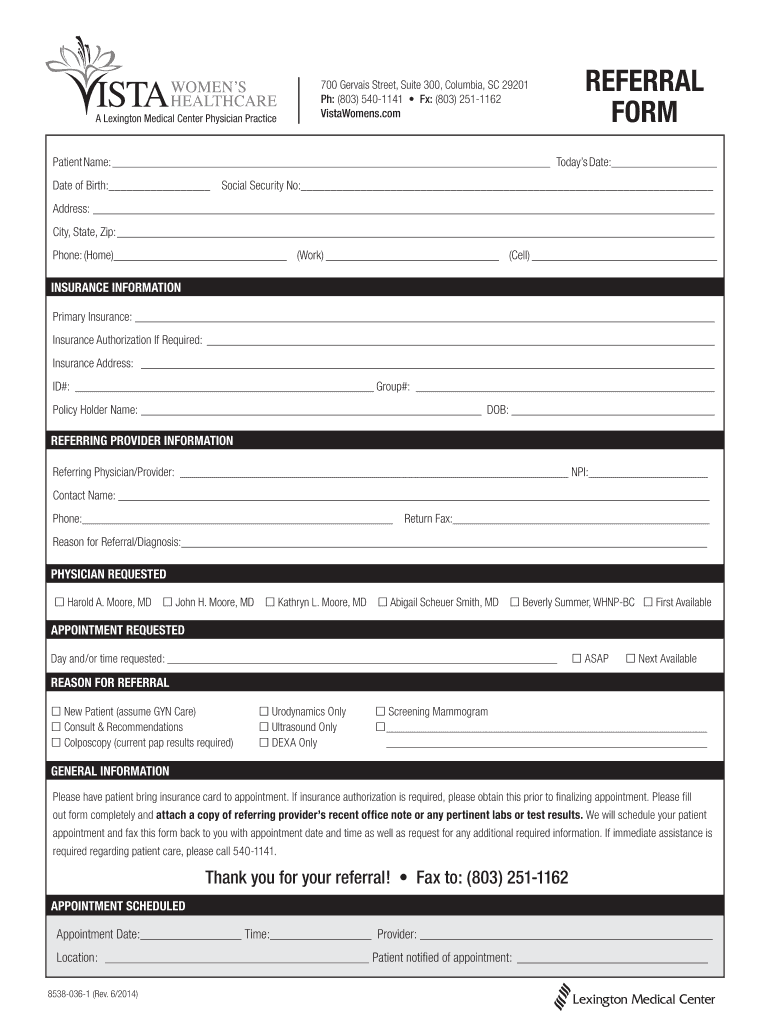
What is Referral Form
The Patient Referral Form is a medical document used by healthcare providers to refer patients to Lexington Medical Center for various medical services.
pdfFiller scores top ratings on review platforms
Who needs Referral Form?
Explore how professionals across industries use pdfFiller.

Referral Form is needed by:
-
Healthcare providers looking to refer patients.
-
Patients needing specialized medical services.
-
Insurance agents coordinating patient care.
-
Administrative staff managing referrals.
-
Medical clinics facilitating patient intake.
Comprehensive Guide to Referral Form
Understanding the Patient Referral Form
The Patient Referral Form is a vital tool in the healthcare process, assisting healthcare providers in referring patients to Lexington Medical Center for various medical services. This healthcare referral form encompasses essential details pertinent to the patient and the reason for their referral. Understanding the purpose and significance of this form ensures a smoother referral process and better patient outcomes.
On this form, providers must input critical information such as patient details and specific reasons for the referral. The Patient Referral Form serves as a bridge between the referring healthcare provider and specialty services, ensuring that both patient needs and medical requirements are met efficiently.
Why Use a Patient Referral Form?
Utilizing a medical referral form streamlines the referral process for healthcare providers, making it easier to collect and organize necessary information efficiently. This contributes to a more effective workflow, enabling healthcare professionals to focus more on patient care and less on administrative tasks.
By ensuring that all crucial information is collected at once, the form can enhance the overall patient experience, potentially impacting timely access to medical services. Proper use of this form also minimizes the chances of errors or miscommunications, thus improving healthcare outcomes.
Key Features of the Patient Referral Form
The Patient Referral Form is designed with several key features that facilitate efficient use. It includes fillable fields for patient information, insurance details, and provider information, ensuring that users can enter all necessary data directly into the document.
-
Checkboxes for selecting requested services and preferred appointment times
-
Clear instructions included for effectively completing the form
-
Ability to save and edit the form online at any point
These functionalities enhance usability and ensure providers have a comprehensive tool at their disposal when referring patients.
Who Should Use the Patient Referral Form?
This form is intended for healthcare providers who need to refer patients within the medical system, including specialists in various fields. Medical professionals ranging from general practitioners to specific specialists can benefit from using this efficient tool to streamline their referral processes.
Additionally, understanding who is eligible for referral is vital to prevent unnecessary delays. The form provides clarity on the types of patients that can be referred based on their medical needs and the services required.
How to Fill Out the Patient Referral Form Online
Filling out the Patient Referral Form online is a simple process that can be accomplished with the following steps:
-
Access the form using your preferred device through pdfFiller.
-
Input patient details, ensuring accuracy in each section.
-
Enter insurance information and the reason for referral clearly.
-
Utilize built-in instructions for any specific sections as needed.
-
Review all details for completeness before submission.
Taking these steps will help ensure that the completed form is accurate and comprehensive, reducing the likelihood of errors that could lead to delays in patient care.
Submission Methods and What to Expect After Submission
Submitting the Patient Referral Form can be done through various methods, including online, fax, or through traditional mail. Each submission method has its own advantages in terms of speed and efficiency, allowing providers to choose the best fit for their practice.
After submission, expect confirmation of receipt from Lexington Medical Center, along with typical processing times for the referral. Understanding what happens next keeps both providers and patients informed and prepared for subsequent steps in the medical process.
Common Errors in the Patient Referral Form and How to Avoid Them
When completing the Patient Referral Form, users should be aware of common errors that could hinder the referral process. Missing information, incorrect insurance details, and unclear referral reasons are frequent pitfalls.
-
Always double-check for completeness before submission
-
Confirm that insurance information is correct and up-to-date
-
Provide clear and specific reasons for the referral to avoid misunderstandings
By following best practices, healthcare providers can significantly reduce the chance of delays caused by incomplete or inaccurate submissions.
Enhancing Security and Compliance with Your Patient Referral Form
Security and compliance are crucial when handling patient information. Using pdfFiller ensures that sensitive data within the Patient Referral Form is managed securely, with robust security measures in place to protect personal information.
Furthermore, the platform adheres to HIPAA and GDPR compliance standards, ensuring that all documentation meets legal requirements. This commitment to security safeguards patient confidentiality, a critical consideration for every healthcare professional.
Utilizing pdfFiller for Your Patient Referral Form Needs
pdfFiller offers a host of advantages for managing your Patient Referral Form. Its user-friendly interface allows for easy online editing and filling of the form, making it accessible to all healthcare providers.
Additionally, benefits like eSigning and secure sharing options facilitate smoother communication between referring providers and specialists, streamlining the referral process further.
Ready to Get Started? Fill Out Your Patient Referral Form Today!
With pdfFiller, you can take advantage of numerous tools designed for ease of use in filling out your Patient Referral Form. By ensuring timely submission, you can enhance overall patient experiences and outcomes. Start using pdfFiller for all your healthcare documentation needs today.
How to fill out the Referral Form
-
1.To access the Patient Referral Form on pdfFiller, visit the pdfFiller website and search for the form using its name or related keywords.
-
2.Once you find the form, click to open it in the editing interface. Familiarize yourself with the layout and navigation options provided by pdfFiller.
-
3.Before you start filling the form, gather all necessary information such as patient details, insurance information, and the reason for referral. Ensure you have specifics about the services requested and preferred appointment times.
-
4.Begin completing the form by clicking on each field to input information. Use checkboxes for the specific services requested and fill in the patient and referring provider details accurately.
-
5.As you fill out the form, pdfFiller allows you to highlight or edit fields easily, ensuring you provide all required information without errors.
-
6.Once all fields are filled, review your entries carefully. Make sure all information is correct, complete, and that you’ve selected the appropriate checkboxes.
-
7.After reviewing, you can finalize your document by saving it within pdfFiller or downloading it to your device. Choose the save or download option according to your needs.
-
8.If needed, you can submit the form directly from pdfFiller or print it for physical submission. Follow the instructions for your preferred submission method.

Who is eligible to use the Patient Referral Form?
The Patient Referral Form is intended for healthcare providers referring patients to Lexington Medical Center for medical services. Eligibility typically includes licensed doctors, nurse practitioners, or medical staff at healthcare facilities.
What information is required to complete the form?
To complete the Patient Referral Form, you will need patient information (name, contact details), insurance details, referring provider’s information, and the reasons for referral. Make sure to have this information ready before filling out the form.
How do I submit the completed Patient Referral Form?
You can submit the completed Patient Referral Form directly through pdfFiller via email or download it for physical submission at Lexington Medical Center. Follow the submission options available in the pdfFiller interface.
Are there deadlines for submitting the Patient Referral Form?
While specific deadlines may vary, it is advisable to submit the Patient Referral Form as soon as possible. Check with Lexington Medical Center for any recommended submission timelines on referrals.
What are common mistakes to avoid when filling out the form?
Common mistakes include incomplete fields, incorrect patient information, and failure to select the appropriate service type. Always double-check all entries before finalizing the form to avoid delays.
How long does it take to process the referral after submission?
The processing time for the referral may vary based on Lexington Medical Center's procedures. Generally, it may take several business days, so follow up if you do not receive confirmation.
Can I edit the Patient Referral Form after saving it?
Yes, once you save the Patient Referral Form in pdfFiller, you can return to it later to make edits. Simply log in to your account, locate the saved form, and make the necessary changes before submitting.
Related Forms





Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.