Medical Authorization Form For Adults








What is a medical authorization form for adults?
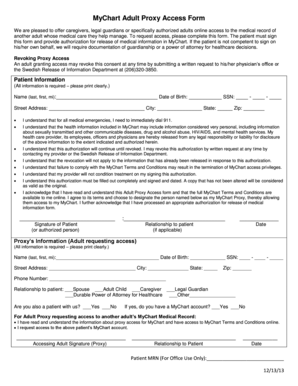
A medical authorization form for adults is a legal document that grants permission to another person or entity to make medical decisions on behalf of an adult individual. This form is essential in situations where the individual is unable to communicate or make decisions due to medical conditions, disabilities, or other circumstances. It ensures that the person's medical needs are still met and allows healthcare professionals to provide necessary treatments and care.
What are the types of medical authorization forms for adults?
There are several types of medical authorization forms for adults, including:
How to complete a medical authorization form for adults
Completing a medical authorization form for adults is a straightforward process. Follow these steps:
pdfFiller is a powerful tool that empowers users to easily create, edit, and share medical authorization forms online. With unlimited fillable templates and robust editing features, pdfFiller simplifies the process of completing and managing important documents, including medical authorization forms. It is the go-to PDF editor that users need to efficiently handle their documentation needs.