Digitally Complete the Medical History Form
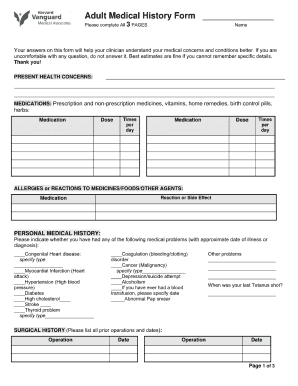
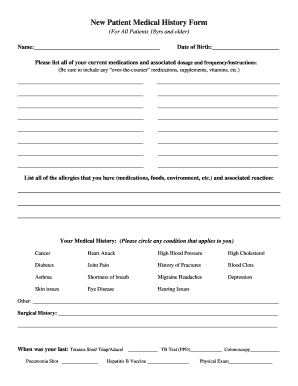
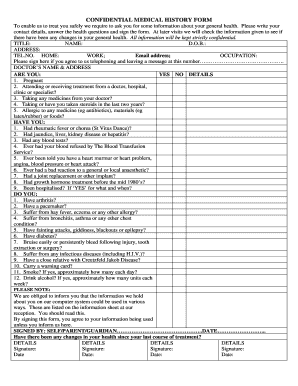
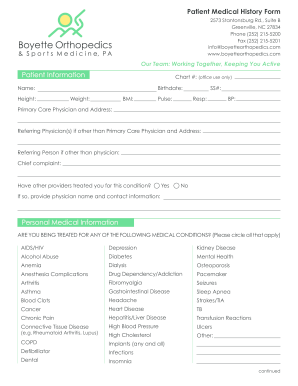
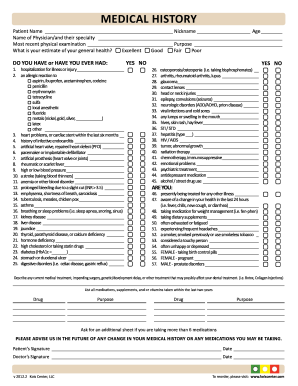
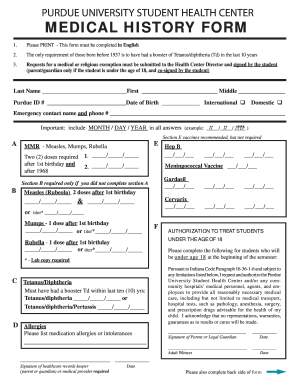
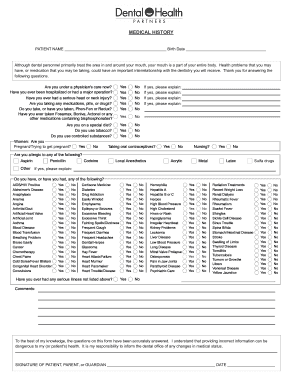
A medical history form is one of the most important documents in regards to your healthcare. It is used to disclose a patient’s medical details to all healthcare providers, ranging from family physicians to dentists. Usually, the doctor needs to know the following information:
Diseases and allergic reactions you have now or have had before.
The recommended medication and treatment used.
Type and frequency of screenings and blood tests.
The patient's personal genetic disposition.
This document is used to help personalize medical treatment between you and your doctor and make sure you receive the most optimal care. The template also provides personal details concerning potential health risks. The sample is extremely useful, and every family member should complete one.
Tips For Creating a Medical History Form
It’s important you provide the most relevant and true-to-life information to the best of your ability. Upload the template, or select one from the PDFfiller library using the search engine. You can easily complete the document by following these instructions:
Read the instructions for every part of the form. Then select the highlighted fields and enter the required data.
The sample you upload will not contain the fillable highlighted fields by default. You need to add them yourself. To do this, go to the "Add Fillable Field" tab and select the "Text" button for name, surname or any other personal details.
If the medical history form requires a marked answer, add a checkmark or an x. Select one of these touls on the upper panel and place it in front of the item you want to select.
Include a signature field and put your initials. Sign your document and send a signature request to your doctor.
In order to protect your personal data, lock the sample with a password. An additional verification check by phone number or social network account may be added as well.