Simple Medical History Form







What is simple medical history form?
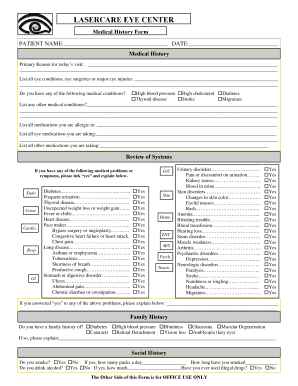
A simple medical history form is a document used by healthcare providers to gather relevant information about a patient's medical background. It includes details such as previous illnesses, surgeries, medications, allergies, and family medical history. By filling out this form, patients provide valuable information to healthcare professionals to help them make informed decisions about their medical care.
What are the types of simple medical history form?
There are several types of simple medical history forms, each designed for specific healthcare settings. Some common types include:
How to complete simple medical history form
Completing a simple medical history form is easy and ensures that healthcare providers have accurate and up-to-date information. To complete the form:
pdfFiller empowers users to create, edit, and share documents online. Offering unlimited fillable templates and powerful editing tools, pdfFiller is the only PDF editor users need to get their documents done.