Last updated on May 20, 2026
CMS-1500 1990-2026 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
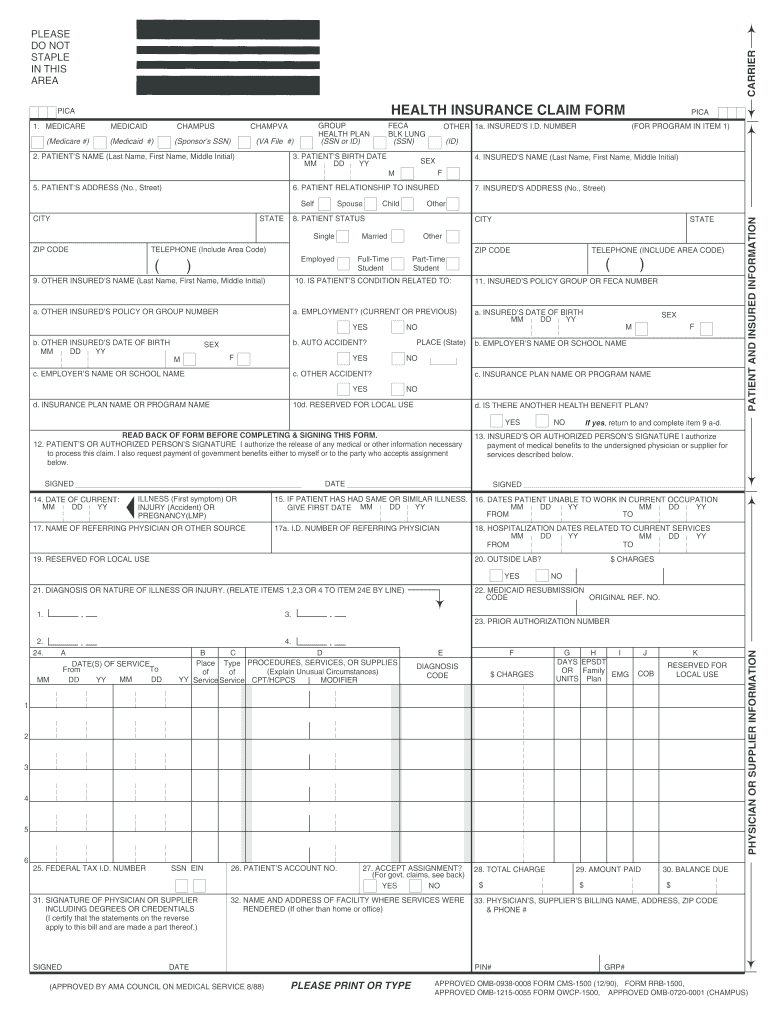
What is CMS-1500
The PICA Health Insurance Claim Form is a healthcare document used by patients and providers to submit claims for medical services to health programs like Medicare and Medicaid.
pdfFiller scores top ratings on review platforms
Who needs CMS-1500?
Explore how professionals across industries use pdfFiller.

CMS-1500 is needed by:
-
Patients seeking reimbursement for healthcare services.
-
Medical providers submitting claims for patient services.
-
Insurance companies processing health claim requests.
-
Healthcare facilities managing billing for services rendered.
-
Administrators handling patient insurance issues.
Comprehensive Guide to CMS-1500
What is the PICA Health Insurance Claim Form?
The PICA Health Insurance Claim Form serves as a crucial document for submitting claims related to various medical services, including those covered by Medicare, Medicaid, and CHAMPUS. This form is essential for facilitating claims in the healthcare ecosystem, ensuring that patients receive the reimbursement they are entitled to for medical treatments.
In essence, the PICA Health Insurance Claim Form includes detailed information about the patient and the services provided. Its role in processing health insurance claims efficiently cannot be overstated.
Purpose and Benefits of the PICA Health Insurance Claim Form
This form is vital for users seeking prompt insurance reimbursement for medical services. By filling out the PICA Health Insurance Claim Form, healthcare providers and patients streamline the process of reimbursement, enhancing the overall efficiency of medical billing.
Using this specific health insurance claim form also reduces the time it takes for claims to be processed, ultimately leading to quicker reimbursement for individuals and medical professionals alike.
Who Needs the PICA Health Insurance Claim Form?
Three primary roles require the PICA Health Insurance Claim Form: Patients, Insured Individuals, and Physicians or Suppliers. Each role plays a significant part in the claims process, making it essential for all involved parties to understand when this form is necessary.
Real-life scenarios where this medical billing form is applicable include instances when a patient receives care from a provider participating in Medicare or Medicaid. Each individual's eligibility will determine the need for completion of this form.
How to Fill Out the PICA Health Insurance Claim Form Online (Step-by-Step)
Filling out the PICA Health Insurance Claim Form online through pdfFiller involves several steps:
-
Access the form and begin with the patient information section.
-
Enter required diagnoses, dates, and service charges in the appropriate fields.
-
Ensure the form includes signatures from the patient, insured, and physician or supplier.
Keep these tips in mind: accurate data entry is essential for successful processing, and verifying that all signatures are present is crucial for authorization.
Common Errors and How to Avoid Them in the PICA Health Insurance Claim Form
Users often encounter pitfalls when completing the PICA Health Insurance Claim Form. Typical errors include:
-
Missing required signatures, which can lead to claim denial.
-
Incorrect or incomplete information that hinders processing.
To avoid these mistakes, it is essential to carefully review all entries before submission and validate the information provided.
Submission Methods and Where to Deliver the PICA Health Insurance Claim Form
Submitting the PICA Health Insurance Claim Form can occur through various methods:
-
Online submission via designated portals.
-
Mailing to the specified address for claims.
-
Faxing to a healthcare provider's billing department.
Be sure to check for any associated fees and submission deadlines ahead of time to ensure timely processing.
What Happens After You Submit the PICA Health Insurance Claim Form?
After submission, the claim enters a processing phase. Users should expect varying processing times depending on the insurance provider. Tracking claims is vital for understanding the status of requests.
If a claim is denied, users should know the common outcomes and their subsequent steps, including appealing the decision if necessary.
Security and Compliance When Using the PICA Health Insurance Claim Form
When handling the PICA Health Insurance Claim Form, confidentiality and data protection are paramount. Security measures such as encryption and HIPAA compliance play a significant role in safeguarding sensitive information during submission.
Always ensure the use of secure platforms for managing documents to maintain compliance and protect personal health data.
Enhance Your Experience with pdfFiller: Quick and Easy Form Management
pdfFiller offers a user-friendly platform for managing the PICA Health Insurance Claim Form. Users can benefit from features such as:
-
Editing documents quickly and efficiently.
-
E-signing forms without the need for downloads.
-
Sharing documents seamlessly through the cloud.
This platform simplifies the entire process of filling out the claim form, making it a preferred choice over traditional methods.
How to fill out the CMS-1500
-
1.To access the PICA Health Insurance Claim Form on pdfFiller, visit the website and use the search bar to locate the form by typing its official name.
-
2.Once the form is displayed, click on it to open it in the pdfFiller interface, where you will find various fillable fields designed for your information.
-
3.Before you begin filling out the form, gather necessary documents such as your insurance card, medical records, and details about the services provided, including dates, diagnoses, and charges.
-
4.As you navigate the form, click on the fillable fields and enter the required information for the patient, insured, and physician or supplier, ensuring all information is accurate and complete.
-
5.Pay close attention to checkboxes and any specific instructions provided, such as reading the back of the form before completing it and signing.
-
6.After filling in all sections of the form, review it for any errors or omissions, confirming that all required signatures are included where indicated.
-
7.Once satisfied with the completed form, use the tools on pdfFiller to save your filled document and choose whether to download it or submit it directly through the platform.

Who is eligible to use the PICA Health Insurance Claim Form?
Eligibility for the PICA Health Insurance Claim Form includes patients who have received medical services covered by Medicare, Medicaid, and other related health programs. Both patients and providers must use the form to claim reimbursement.
What documents are needed to fill out the form?
To complete the PICA Health Insurance Claim Form, you will need your health insurance card, documentation of the medical services received, including dates, diagnoses, and charges, as well as any other supportive documents relevant to the claim.
How can I submit the completed form?
After filling out the PICA Health Insurance Claim Form, it can be submitted by mailing it to your insurance company, or you may use online portals such as pdfFiller for direct submission via email or print. Always check for specific submission procedures required by your insurer.
What are common mistakes to avoid when filling out the form?
Common mistakes include omitting signatures, failing to provide complete information, and neglecting to review the back of the form for additional instructions. Double-check your entries and ensure all required fields are filled before submission.
Are there any deadlines for submitting the PICA Health Insurance Claim Form?
Most health programs have specific deadlines for submitting claims, typically ranging from 90 days to a year after the service date. Check with your insurance provider for their specific submission deadlines to ensure claims are processed timely.
How long does processing of claims usually take?
Processing times for health insurance claims can vary widely based on the insurer, but generally, it ranges from 2 to 6 weeks. It's advisable to follow up with your insurance provider if confirmation is not received within this period.
What should I do if my claim is denied?
If your claim is denied, review the denial notice for specific reasons. You can appeal the decision by providing additional documentation or clarifications, and it's often beneficial to contact your health insurance representative for assistance throughout the appeal process.
Related Content
Related Forms




Related Catalogs
Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.