Last updated on May 26, 2026
GA DMA-6A 2004 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
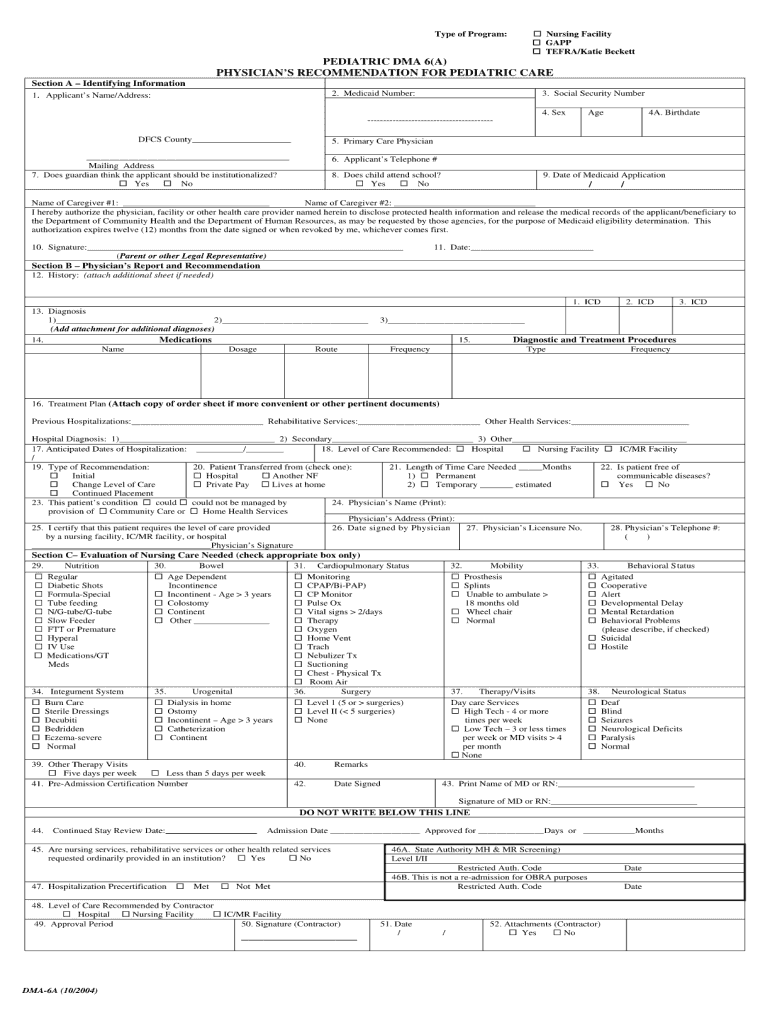
What is GA DMA-6A
The GA DMA-6A is a document used by authorized entities to report certain tax-related information in Georgia. Its primary purpose is to ensure compliance with state tax regulations.
pdfFiller scores top ratings on review platforms
The best thing that I can say about PDFFiller is that it is easy to use.
WORKS GREAT
Great format. Easy to use. Good price.
It fills out PDF's easily.
Very easy to use and discover the tools fuctionality. Perfect!!
Great Service
Who needs GA DMA-6A?
Explore how professionals across industries use pdfFiller.

GA DMA-6A is needed by:
-
Tax professionals managing client submissions in Georgia
-
Businesses operating in Georgia that must report tax information
-
Accounting firms preparing documentation for state compliance
-
Individuals seeking to verify their tax-related obligations
-
Consultants advising on Georgia tax compliance
Comprehensive Guide to GA DMA-6A
What is the GA DMA-6A?
The GA DMA-6A form serves a crucial role in the realm of document management. This form is essential for meeting the requirements associated with filing and managing documents efficiently. The GA DMA-6A aids in streamlining organization and accessibility across various fields.
It functions as a standardized document that ensures compliance with regulatory needs, making it significant for users who prioritize effective filing practices. Understanding its purpose is vital for anyone involved in document management.
Purpose and Benefits of the GA DMA-6A
The GA DMA-6A is not merely a form; it is a valuable asset designed to enhance organizational efficiency and compliance. Situations that necessitate the GA DMA-6A often involve regulatory submissions where clear documentation is essential.
By utilizing this form, users can expect benefits such as improved compliance with legal requirements, enhanced organizational capabilities, and the potential for cost savings on administrative processes.
Who Needs the GA DMA-6A?
Identifying the target audience for the GA DMA-6A is key to ensuring its effective use. This form is typically required by professionals and organizations involved in various sectors that necessitate robust document management.
Eligible filers include businesses, government entities, and individuals responsible for submitting important documentation. Understanding who needs this form can lead to better compliance and organization.
How to Fill Out the GA DMA-6A Online (Step-by-Step)
Completing the GA DMA-6A online is straightforward and can be achieved efficiently with pdfFiller. Follow these steps to fill out the form:
-
Access the GA DMA-6A form through pdfFiller’s platform.
-
Edit the template directly in your browser using the editing tools available.
-
Include all required information accurately.
-
Utilize the eSigning feature to sign the document electronically.
-
Save and submit the completed form as per the submission guidelines.
These steps emphasize the ease of use when filling out the GA DMA-6A online, ensuring a smooth process.
Key Features of pdfFiller for Completing the GA DMA-6A
pdfFiller offers several features that significantly enhance the form-filling process for the GA DMA-6A. Key features include:
-
Editing capabilities for text and images, allowing users to tailor the document as needed.
-
E-signature options, which provide a quick and easy way to sign documents.
-
Annotation tools for making notes or comments directly on the form.
-
Cloud-based storage that ensures document security and easy access.
These capabilities not only streamline the completion of the GA DMA-6A but also provide reassurance through robust security measures for handling sensitive information.
Common Errors and How to Avoid Them while Submitting the GA DMA-6A
Users often encounter common errors when filling out the GA DMA-6A, which can impede a successful submission. Some frequent mistakes include:
-
Inaccurate personal or business information entered into the form.
-
Failure to sign or date the document properly.
-
Omission of required fields that could lead to rejection.
To minimize mistakes, it is advisable to double-check the completed form for accuracy, ensure all necessary fields are filled out, and utilize available resources for clarification as needed.
Where to Submit the GA DMA-6A and Important Deadlines
Understanding the correct submission methods for the GA DMA-6A is essential for timely compliance. Accepted submission methods include:
-
Submitting via physical mail to the designated address.
-
Emailing the completed form to the appropriate office.
Additionally, it is crucial to be aware of submission deadlines and processing time frames to avoid potential complications with the filing.
Security and Compliance for the GA DMA-6A
When dealing with sensitive documents such as the GA DMA-6A, security and compliance are paramount. pdfFiller implements stringent security measures, including:
-
256-bit encryption to protect user data during transfer and storage.
-
Compliance with regulations such as HIPAA and GDPR, ensuring data privacy.
These protocols are designed to build user trust and ensure that sensitive information is handled with the utmost care.
Final Steps After Submitting the GA DMA-6A
After submitting the GA DMA-6A, users should be prepared for the subsequent steps in the application process. It is important to know how to check the status of your submission.
Typically, users receive an acknowledgment of submission, followed by updates on processing details. Being informed about the timeline can help in managing expectations effectively.
Utilize pdfFiller to Complete Your GA DMA-6A Form Efficiently
Leveraging pdfFiller for completing the GA DMA-6A form offers users a reliable and efficient solution. By using this platform, individuals can take advantage of numerous features that facilitate effective document management.
Utilizing a trusted platform like pdfFiller not only expedites the form submission process but also ensures security and compliance throughout.
How to fill out the GA DMA-6A
-
1.To access the GA DMA-6A form on pdfFiller, visit the pdfFiller website and use the search bar to find the specific form by name.
-
2.Once you locate the form, click on it to open the editable document within the pdfFiller interface.
-
3.Before filling out the form, gather all necessary information such as tax identification numbers, financial records, and relevant transaction details to ensure accurate completion.
-
4.Begin filling out the form by clicking on each field to enter the required information. Note the placeholder text for guidance on what to input.
-
5.If you need to make changes, use the tools provided in pdfFiller to edit, delete, or add text as necessary. Take advantage of features like spell check to minimize errors.
-
6.Review the completed form carefully, ensuring that all fields are filled correctly and that your information is accurate to avoid processing delays.
-
7.After finalizing your entries, utilize the options available to save or download the form directly from pdfFiller. You can also submit it online if applicable.

Who is eligible to use the GA DMA-6A form?
The GA DMA-6A form is primarily intended for businesses and tax professionals operating in Georgia. Individuals may also use it to ensure compliance with state tax regulations.
What are the submission methods for the GA DMA-6A?
The GA DMA-6A can typically be submitted online via the Georgia Department of Revenue's portal or mailed directly to the specified address on the form.
Are there deadlines associated with filing the GA DMA-6A?
It is essential to check the specific deadlines outlined by the Georgia Department of Revenue, as these can vary based on the type of submission and fiscal year.
What common mistakes should be avoided when completing the GA DMA-6A?
Ensure all fields are correctly filled and double-check for any typos, particularly in identification numbers, as inaccuracies can lead to delays or rejection of the form.
What supporting documents are required for filing the GA DMA-6A?
Supporting documents may include financial records, previous tax forms, and any correspondence with the Georgia Department of Revenue. It's advisable to include all relevant documentation to support your submission.
How long does processing take for the GA DMA-6A?
Processing times for the GA DMA-6A can vary. It's often best to allow several weeks for the form to be processed, so plan submissions well in advance of any deadlines.
What should I do if I need to make changes after submitting the GA DMA-6A?
If you need to amend the GA DMA-6A after submission, contact the Georgia Department of Revenue directly for guidance on the required process to update your information.
GA DMA-6A Form Versions
Related Content
Related Forms
Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.