Last updated on May 20, 2026
OCA Official Form 930 NYHIPAA 2009-2026 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
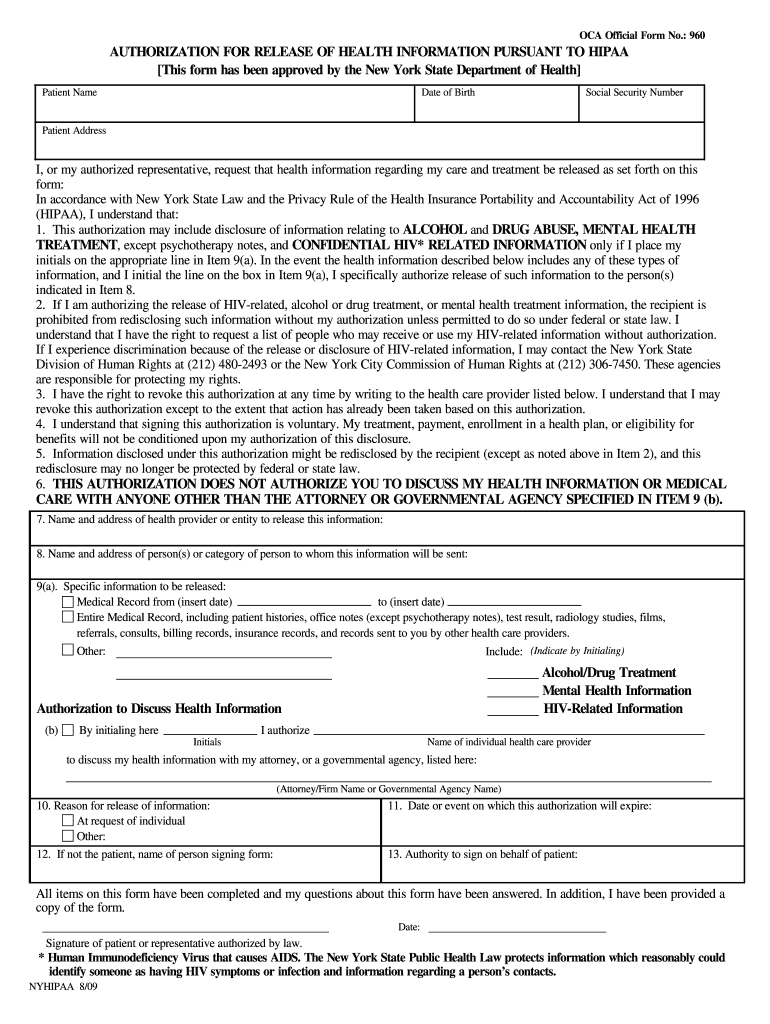
What is OCA Official Form 930 NYHIPAA
The New York HIPAA Authorization for Release of Health Information is a legal document used by patients or their authorized representatives to request the release of health information for various purposes.
pdfFiller scores top ratings on review platforms
I have only been using PDFfiller for a couple of months but it has been a godsend. My son has 3 different court cases going and that is a ton of forms that need to be filled out every time he needs to file or respond. PDFfiller makes the process extremely easy. All I do is search the form, add it to my profile and then fill it out. It retains ALL the information and adds it to the next page so that I am not having to repeat the same information over and over. This is all I have used it for but am looking forward to what other features I will be able to use in the future.
I found PDFfiller very useful for making changes to a financial statement that evolved as circumstances changed.
Who needs OCA Official Form 930 NYHIPAA?
Explore how professionals across industries use pdfFiller.

OCA Official Form 930 NYHIPAA is needed by:
-
Patients seeking access to their medical records
-
Authorized representatives managing patient health information
-
Healthcare providers requiring patient consent for information disclosure
-
Legal professionals handling health-related litigation
-
Mental health professionals managing sensitive information
-
Substance abuse counselors working with patient data
Comprehensive Guide to OCA Official Form 930 NYHIPAA
What is the New York HIPAA Authorization for Release of Health Information?
The New York HIPAA Authorization for Release of Health Information is a crucial form in healthcare management. This authorization is legally defined as a document allowing patients or their authorized representatives to request specified health information, including medical records and mental health information. The form serves as a legal authority that ensures compliance with HIPAA regulations, protecting patient data while allowing necessary information sharing.
This authorization can be used for a variety of health information purposes, including for legal proceedings, patient care, or personal reasons. It facilitates the release of specific health data deemed necessary for these scenarios.
Purpose and Benefits of the New York HIPAA Authorization for Release of Health Information
The primary purpose of this authorization is to ensure the legal and compliant transfer of health information. By utilizing the New York health release, patients can access their medical histories to support legal, medical, or personal needs. This form provides clear benefits in various situations such as litigation or obtaining second opinions from healthcare providers.
Ensuring compliance with HIPAA regulations is paramount when sharing health information, as it protects both the patient's rights and the healthcare provider involved in the process.
Key Features of the New York HIPAA Authorization for Release of Health Information
The authorization form contains several essential components that users should be aware of. Fillable fields include:
-
Patient information
-
Recipient of the information
-
Purpose for the information release
This form also outlines signature requirements, indicating that both patients and their authorized representatives must sign for it to be valid. Additionally, it specifies expiration date provisions and identifies the types of health information that can be released under this authorization.
Who Needs the New York HIPAA Authorization for Release of Health Information?
Various individuals or roles may require this form. Patients may need it for situations like transferring their records or reviewing past medical treatments. Authorized representatives play a significant role in this authorization process, especially in cases where patients are unable to sign for themselves.
Examples of scenarios requiring the authorization include when patients seek second opinions, partake in litigation processes, or require coordinated care between different healthcare providers.
How to Fill Out the New York HIPAA Authorization for Release of Health Information Online
Completing the authorization form online is straightforward. Here’s a step-by-step guide to filling out the form:
-
Access the New York HIPAA authorization form via pdfFiller.
-
Fill in the patient’s personal information, including name and contact details.
-
Specify the recipient of the health information.
-
Indicate the purpose for the request.
-
Review the completed form for any errors or missing information.
To ensure the form is filled out correctly, avoid common mistakes such as incomplete fields or neglecting to provide a signature. Verify each detail aligns with HIPAA guidelines to maintain compliance throughout the process.
How to Sign the New York HIPAA Authorization for Release of Health Information
Signing the New York HIPAA Authorization can be done through both digital and traditional methods. Digital signatures offer convenience and quick processing, particularly through platforms like pdfFiller.
When using electronic signatures, follow these instructions:
-
Select the eSign option within the pdfFiller interface.
-
Complete the signature as prompted, ensuring it meets legal standards.
It is important to remember that valid signatures are essential for the authorization to be legally binding, regardless of whether they are digital or traditional wet signatures.
Where and How to Submit the New York HIPAA Authorization for Release of Health Information
Submitting the authorization form is an essential step in the process. Users can submit the form through various methods, including:
-
Online submission via pdfFiller
-
Mailing the form directly to the healthcare provider
-
Delivers in person at the healthcare facility
After submission, it's helpful to know what entities may require this authorization and the expected timelines for processing requests and receiving the requested health information.
Security and Compliance Considerations for the New York HIPAA Authorization
Ensuring the security of health information is pivotal in handling the New York HIPAA Authorization. Compliance with HIPAA regulations protects patient data and promotes trust in healthcare systems. Important security measures include:
-
Use of 256-bit encryption to safeguard data
-
Adhering to SOC 2 Type II standards to verify operational security
Additionally, organizations must follow record retention requirements after the form is submitted to comply with legal obligations regarding patient information.
How pdfFiller Can Help You with the New York HIPAA Authorization for Release of Health Information
pdfFiller provides valuable assistance in completing the New York HIPAA Authorization. Users can benefit from features that include:
-
Fillable forms that simplify the input process
-
Effortless eSigning to ensure compliance
-
User-friendly interface that eases document management
Moreover, pdfFiller guarantees data security during the handling and submission of sensitive documents, reassuring users of their information's privacy and protection.
Filling Out Your New York HIPAA Authorization Form: Next Steps
Now that you are equipped with the knowledge to fill out your New York HIPAA Authorization form, consider starting the process using pdfFiller's tools. Support resources are readily available for any assistance needed during completion. pdfFiller enhances accessibility and management of health documents, streamlining the entire experience.
How to fill out the OCA Official Form 930 NYHIPAA
-
1.Access the New York HIPAA Authorization form on pdfFiller by searching 'HIPAA Authorization for Release of Health Information' in the search bar.
-
2.Open the form to begin filling it out. Familiarize yourself with the layout and the locations of each required field.
-
3.Before you start, gather important information such as the patient's full name, date of birth, social security number, and address, as well as details about the health provider and recipient.
-
4.Fill in the 'Patient Name', 'Date of Birth', 'Social Security Number', and 'Patient Address' fields on the form as prompted.
-
5.Use the checkboxes to indicate specific health information that needs to be released, including medical records, mental health information, or details about substance abuse treatment.
-
6.If needed, add the name and details of the health provider and the person who will receive the information in the designated fields.
-
7.Specify the reason for the release of information and enter an expiration date or event for the authorization if applicable.
-
8.Review all filled entries to ensure accuracy before signing. Check that all necessary fields are completed and that signatures are in place.
-
9.Once you have reviewed the entire document, follow pdfFiller's instructions to save your progress.
-
10.You can choose to download the completed form as a PDF or submit it electronically through the platform, following any additional submission instructions provided.

Who is eligible to use the New York HIPAA Authorization form?
The form can be used by any patient in New York wanting to authorize the release of their health information, as well as their authorized representatives.
How long is the authorization valid?
The authorization remains valid until the expiration date stated on the form or until the purpose for the authorization is fulfilled, whichever comes first.
What information is needed when filling out the form?
You will need the patient’s name, date of birth, social security number, address, details about the healthcare provider, the recipient of the information, and the reason for the request.
Are there any submission methods available for the completed form?
Completed forms can typically be submitted directly to the healthcare provider or authorized recipient, and you may use pdfFiller's options to download or send electronically.
What are common mistakes to avoid when completing this form?
Ensure that all required fields are filled correctly, avoid leaving any blank spaces, double-check that signatures are provided, and verify that the correct information is being released.
Is notarization required for this form?
No, notarization is not required for the New York HIPAA Authorization for Release of Health Information.
What should I do if I need help filling out the form?
If you need assistance, you can reach out to healthcare providers for guidance or consult with legal professionals specializing in health information privacy.
Related Content
Related Forms






Related Catalogs
Get the latest insights from our blog

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.