Last updated on Jun 2, 2026
Instructions on How to Fill Out the CMS 1500 Form 2008-2026 free printable template
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
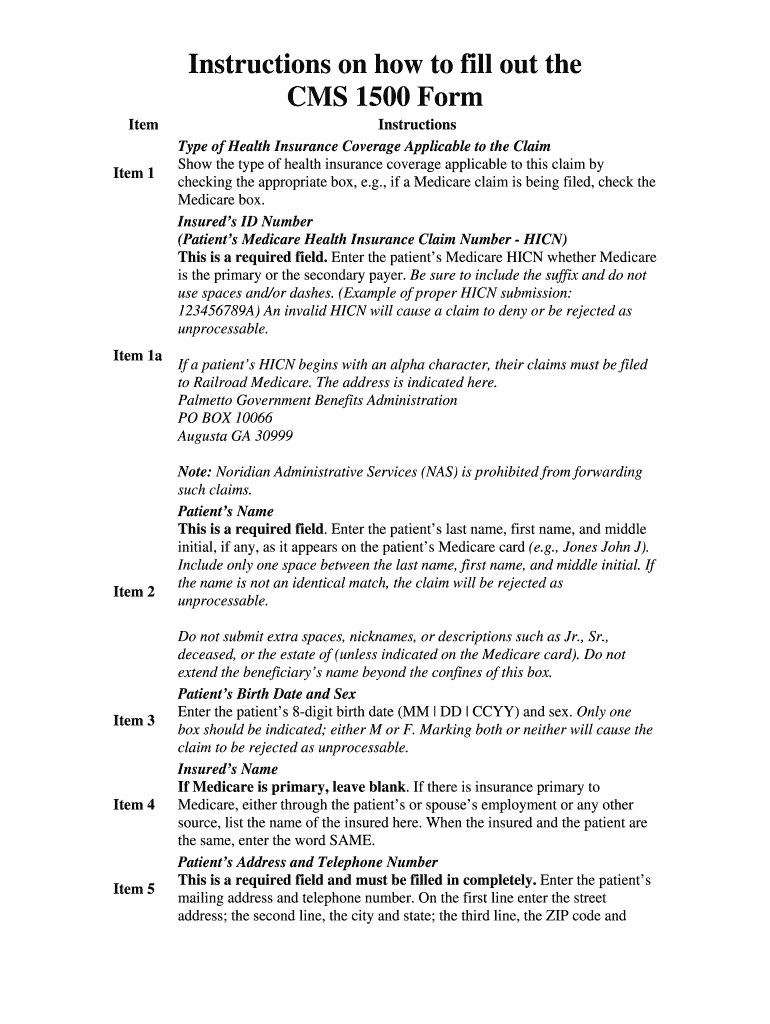
What is Instructions on How to Fill Out the CMS 1500 Form
The CMS 1500 Form Instructions is a type of instructional document used by healthcare providers and patients to accurately complete the CMS 1500 Form for Medicare claims.
pdfFiller scores top ratings on review platforms
Who needs Instructions on How to Fill Out the CMS 1500 Form?
Explore how professionals across industries use pdfFiller.

Instructions on How to Fill Out the CMS 1500 Form is needed by:
-
Patients seeking to file Medicare claims
-
Physicians or healthcare providers submitting claims
-
Medigap insurers reviewing patient claims
-
Medical billing specialists and offices
-
Healthcare administrators handling paperwork
Comprehensive Guide to Instructions on How to Fill Out the CMS 1500 Form
What is the CMS 1500 Form?
The CMS 1500 Form is a vital document used for submitting Medicare claims. Its primary purpose is to facilitate the reimbursement process for healthcare providers by accurately detailing patient services. Ensuring accurate completion is crucial, as it directly impacts both healthcare providers and patients, ensuring timely payment and reducing claim denials.
Purpose and Benefits of the CMS 1500 Form Instructions
The CMS 1500 Form Instructions serve as a comprehensive guide designed for both healthcare providers and patients. Understanding these instructions can streamline the claims processing, minimizing errors that lead to delays. By clearly outlining the necessary steps and information, this guide ultimately benefits all parties involved in the claims submission process.
Key Features of the CMS 1500 Form Instructions
These instructions include critical information on various aspects of the form. Key features consist of:
-
Detailed descriptions of required patient information
-
Guidelines for Medigap benefits
-
Clarifications on common errors to avoid
Who Needs the CMS 1500 Form?
Three main entities primarily utilize the CMS 1500 Form: patients, physicians/suppliers, and Medigap insurers. Each party has a unique role; patients must provide personal information, physicians/suppliers complete the medical details, and Medigap insurers review the claims for benefits. Accurate collaboration among these groups is key to effective claims submission.
How to Fill Out the CMS 1500 Form Instructions Online
Filling out the CMS 1500 Form online can be accomplished through user-friendly platforms like pdfFiller. The step-by-step process to complete the form includes:
-
Access the CMS 1500 Form template on pdfFiller.
-
Fill in the required patient and insurance details.
-
Utilize editing tools to ensure accuracy.
-
eSign the document if required.
-
Submit the completed form through the chosen method.
Field-by-Field Instructions for the CMS 1500 Form
This section provides a detailed explanation of each field on the CMS 1500 Form. Important fields include:
-
Patient’s name and birth date
-
Insurance policy details
-
Employment status information
Common pitfalls include incorrect coding or missing information, which can lead to claim delays.
When and Where to Submit the CMS 1500 Form
Timely submission of the CMS 1500 Form is essential for successful claims processing. Key aspects of submission include:
-
Understanding submission deadlines for timely filing
-
Identifying acceptable submission methods, including both online and offline options
Common Issues When Filing CMS 1500 Forms
Claim denials can occur for several reasons. Common issues include:
-
Missing patient information
-
Incorrect procedure codes
-
Late filing or necessary resubmission procedures
Being aware of these problems can help in avoiding pitfalls during the claims submissions process.
Security and Privacy Considerations
It is critical to secure sensitive patient information during the claims process. pdfFiller emphasizes security with measures such as:
-
256-bit encryption
-
Compliance with HIPAA and GDPR regulations
-
Regular security audits to protect user data
Maximize Your CMS 1500 Form Experience with pdfFiller
Using pdfFiller for filling out the CMS 1500 Form can greatly enhance the user experience. Features that can be particularly helpful include:
-
Editing and annotating capabilities
-
eSigning options
-
Cloud-based access for easy form management
These features collectively create a more efficient and seamless form handling experience.
How to fill out the Instructions on How to Fill Out the CMS 1500 Form
-
1.Access the CMS 1500 Form Instructions on pdfFiller by searching for its title in the form library.
-
2.Open the document to familiarize yourself with the layout and required fields.
-
3.Gather necessary information including the patient's name, birth date, address, and insurance details.
-
4.Follow the instructions outlined in the document, focusing on each section individually.
-
5.Use the text fields on pdfFiller to input details as per the instructions for each line of the form.
-
6.Pay special attention to sections related to Medigap benefits and insurance information.
-
7.After filling in all required fields, review the document for any errors or omissions.
-
8.Finalize your form by using the pdfFiller tools to check corrections and adjustments.
-
9.Save your completed form in the desired format. You can also download it or submit it directly through pdfFiller.

What are the eligibility requirements for using the CMS 1500 Form?
To use the CMS 1500 Form, patients must be enrolled in Medicare, and the claims must relate to services covered under this program.
What is the deadline for submitting the CMS 1500 Form?
There is typically no specific deadline, but it is advisable to submit Medicare claims within one year of receiving services to ensure timely processing.
How can I submit the CMS 1500 Form?
The CMS 1500 Form can be submitted electronically through a claims management system, or physically mailed to the appropriate Medicare contractor.
What supporting documents are required with the CMS 1500 Form?
You may need additional documents such as medical records, proof of services rendered, and an explanation of benefits from secondary insurance.
What are common mistakes to avoid when filling out the CMS 1500 Form?
Common mistakes include incomplete fields, incorrect patient identification numbers, and not signing where required by the patient or authorized representative.
How long does processing of the CMS 1500 Form take?
Processing times vary, but Medicare usually takes about 30 days to process claims submitted on the CMS 1500 Form.
Are there any fees associated with submitting the CMS 1500 Form?
Typically, there are no fees for submitting the CMS 1500 Form itself, but healthcare providers may charge for their services related to the claim submission.
Related Content
Related Forms



Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.