Add or replace text, adjust formatting, insert legally binding eSignatures, and send documents for signing without hopping between apps.

CMS-1500 UB-04 CMS-1450 Package free printable template
Show details
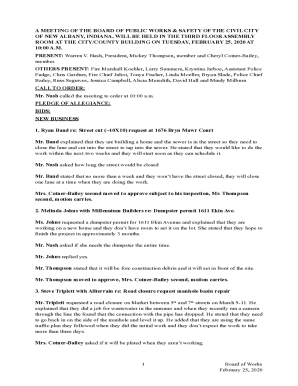
CARRIER HEALTH INSURANCE CLAIM FORM APPROVED BY NATIONAL UNIFORM CLAIM COMMITTEE 08/05 PICA MEDICARE MEDICAID Medicare TRICARE CHAMPUS Sponsor s SSN Medicaid GROUP HEALTH PLAN SSN or ID CHAMPVA Member ID 3. AUTO ACCIDENT PLACE State c. OTHER ACCIDENT c. INSURANCE PLAN NAME OR PROGRAM NAME NO YES d. IS THERE ANOTHER HEALTH BENEFIT PLAN 10d. RESERVED FOR LOCAL USE READ BACK OF FORM BEFORE COMPLETING SIGNING THIS FORM. 12. PATIENT S OR AUTHORIZED PERSON S SIGNATURE I authorize the release of any...medical or other information necessary to process this claim. I also request payment of government benefits either to myself or to the party who accepts assignment below. PRIOR AUTHORIZATION NUMBER 24. A. BECAUSE THIS FORM IS USED BY VARIOUS GOVERNMENT AND PRIVATE HEALTH PROGRAMS SEE SEPARATE INSTRUCTIONS ISSUED BY APPLICABLE PROGRAMS. NOTICE Any person who knowingly files a statement of claim containing any misrepresentation or any false incomplete or misleading information may be guilty of a...criminal act punishable under law and may be subject to civil penalties. REFERS TO GOVERNMENT PROGRAMS ONLY MEDICARE AND CHAMPUS PAYMENTS A patient s signature requests that payment be made and authorizes release of any information necessary to process the claim and certifies that the information provided in Blocks 1 through 12 is true accurate and complete. In the case of a Medicare claim the patient s signature authorizes any entity to release to Medicare medical and nonmedical information...including employment status and whether the person has employer group health insurance liability no-fault worker s compensation or other insurance which is responsible to pay for the services for which the Medicare claim is made. 8. For Medicaid purposes The submitter understands that because payment and satisfaction of this claim will be from Federal and State funds any false statements documents or concealment of a material fact are subject to prosecution under applicable Federal or State...Laws. 9. For TRICARE Purposes complete to the best of the submitter s knowledge and belief and services were medically necessary and appropriate for the health of the patient b The patient has represented that by a reported residential address outside a military medical treatment facility catchment area he or she does not live within the catchment area of a U.S. military medical treatment facility or if the patient resides within a catchment area of such a facility a copy of Non-Availability...Statement DD Form 1251 is on file or the physician has certified to a medical emergency in any instance where a copy of a NonAvailability Statement is not on file c The patient or the patient s parent or guardian has responded directly to the provider s request to identify all health insurance coverage and that all such coverage is identified on the face of the claim except that coverage which is exclusively supplemental payments to TRICARE-determined benefits d The amount billed to TRICARE has...been billed after all such coverage have been billed and paid excluding Medicaid and the amount billed to TRICARE is that remaining claimed against TRICARE benefits e The beneficiary s cost share has not been waived by consent or failure to exercise generally accepted billing and collection efforts and f Any hospital-based physician under contract the cost of whose services are allocated in the charges included in this bill is not an employee or member of the Uniformed Services. For purposes of...this certification an employee of the Uniformed Services is an employee appointed in civil service refer to 5 USC 2105 including part-time or intermittent employees but excluding contract surgeons or other personal service contracts. 9. For TRICARE Purposes complete to the best of the submitter s knowledge and belief and services were medically necessary and appropriate for the health of the patient b The patient has represented that by a reported residential address outside a military medical...treatment facility catchment area he or she does not live within the catchment area of a U.S. military medical treatment facility or if the patient resides within a catchment area of such a facility a copy of Non-Availability Statement DD Form 1251 is on file or the physician has certified to a medical emergency in any instance where a copy of a NonAvailability Statement is not on file c The patient or the patient s parent or guardian has responded directly to the provider s request to identify...all health insurance coverage and that all such coverage is identified on the face of the claim except that coverage which is exclusively supplemental payments to TRICARE-determined benefits d The amount billed to TRICARE has been billed after all such coverage have been billed and paid excluding Medicaid and the amount billed to TRICARE is that remaining claimed against TRICARE benefits e The beneficiary s cost share has not been waived by consent or failure to exercise generally accepted...billing and collection efforts and f Any hospital-based physician under contract the cost of whose services are allocated in the charges included in this bill is not an employee or member of the Uniformed Services. For purposes of this certification an employee of the Uniformed Services is an employee appointed in civil service refer to 5 USC 2105 including part-time or intermittent employees but excluding contract surgeons or other personal service contracts. Similarly member of the Uniformed...Services does not apply to reserve g Based on 42 United States Code 1395cc a 1 j all providers participating in Medicare must also participate in TRICARE for inpatient hospital services provided pursuant to admissions to hospitals occurring on or after January 1 1987 and h If TRICARE benefits are to be paid in a participating status the submitter of this claim agrees to submit this claim to the appropriate TRICARE claims processor. The patient s signature on the provider s request to bill...Medicare medical and non-medical information including employment status and whether the person has employer group health insurance which is responsible to pay for the services for which this Medicare claim is made. 8. For Medicaid purposes The submitter understands that because payment and satisfaction of this claim will be from Federal and State funds any false statements documents or concealment of a material fact are subject to prosecution under applicable Federal or State Laws. 9. For...TRICARE Purposes complete to the best of the submitter s knowledge and belief and services were medically necessary and appropriate for the health of the patient b The patient has represented that by a reported residential address outside a military medical treatment facility catchment area he or she does not live within the catchment area of a U.S. military medical treatment facility or if the patient resides within a catchment area of such a facility a copy of Non-Availability Statement DD...Form 1251 is on file or the physician has certified to a medical emergency in any instance where a copy of a NonAvailability Statement is not on file c The patient or the patient s parent or guardian has responded directly to the provider s request to identify all health insurance coverage and that all such coverage is identified on the face of the claim except that coverage which is exclusively supplemental payments to TRICARE-determined benefits d The amount billed to TRICARE has been billed...after all such coverage have been billed and paid excluding Medicaid and the amount billed to TRICARE is that remaining claimed against TRICARE benefits e The beneficiary s cost share has not been waived by consent or failure to exercise generally accepted billing and collection efforts and f Any hospital-based physician under contract the cost of whose services are allocated in the charges included in this bill is not an employee or member of the Uniformed Services.
We are not affiliated with any brand or entity on this form
Fill out, sign, and share forms from a single PDF platform
Manage all your documents quickly and securely in the cloud.
Edit and sign in one place
Create professional forms
Add and customize fillable fields to tailor each form to your needs and ensure easy completion without printing and scanning.
Simplify data collection
Quickly share forms via email or a secure link, enabling anyone to complete forms online in seconds, on any device.
Manage forms centrally
Keep all your forms and templates organized in one secure, cloud-based platform, track changes easily, and export documents in any format.


Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
Understanding the CMS-1500 UB-04 CMS-1450 Package Form
What is the CMS-1500 UB-04 CMS-1450 Package Form?
The CMS-1500 UB-04 CMS-1450 package form is a unified document used for submitting health insurance claims in the United States. It is designed for healthcare providers to report services rendered to patients and for insurers to process these claims efficiently. The form combines two essential formats, making it suitable for various billing scenarios, including traditional and electronic submissions.
Key Features of the CMS-1500 UB-04 CMS-1450 Package Form
This form features several critical components that streamline claims processing. Key elements include:
-
Helps separate important information regarding patient details, services provided, and billing codes.
-
Facilitates submission through various digital platforms, reducing processing time.
-
Accommodates multiple medical code systems, allowing for accurate service descriptions.
-
Ensures comprehensive data collection on both patients and healthcare providers.
How to Fill the CMS-1500 UB-04 CMS-1450 Package Form
When completing this form, attention to detail is crucial. Users should follow these steps:
-
Fill in the patient’s name, date of birth, and ID information accurately.
-
Input the primary insurer's information, including the policy number.
-
Use CPT/HCPCS codes to describe each service provided during the patient’s care.
-
Utilize appropriate ICD-10 codes to represent the patient’s diagnosis accurately.
Common Errors and Troubleshooting
Completing the CMS-1500 UB-04 CMS-1450 form can sometimes lead to errors, which may result in claim rejections. Common mistakes include:
-
Always double-check names and identification numbers for accuracy.
-
Ensure that all codes match the services and diagnoses related to the claim.
-
A signature is necessary to authorize the release of medical information and claims.
-
Attach necessary documents to support claims, such as medical records or referrals.
Benefits of Using the CMS-1500 UB-04 CMS-1450 Package Form
Utilizing this comprehensive package form presents several benefits for healthcare providers, including:
-
Offers a standardized approach that simplifies the claims process.
-
Reduces timeframes for reimbursement due to streamlined information.
-
Allows providers to maintain clear and organized records for auditing and review.
Who Needs the CMS-1500 UB-04 CMS-1450 Package Form
This form is essential for various stakeholders in the healthcare industry, primarily:
-
Doctors, clinics, and hospitals that render services and need to bill for them.
-
Entities responsible for processing medical claims for reimbursement.
-
Individuals who require documentation for their health services and to submit for claims.
Frequently Asked Questions about cms 1500 form
What type of claims can be submitted using the CMS-1500 UB-04 CMS-1450 package form?
The form can be used for a variety of health insurance claims, including those related to outpatient services and office visits across various specialties.
Is electronic filing available for the CMS-1500 UB-04 CMS-1450 package form?
Yes, the form is compatible for electronic filing, allowing for expedited processing and tracking within insurance systems.
pdfFiller scores top ratings on review platforms
I have only been using a few days give me time and I will let you know.
its been a good one except when a have a parallel page and i need it to be vertical i cannot rotate it. (I tried)
You made it so easy and I did not have to pay my accountant to do it. Thank you.
It's easy to use, I do like it; but it is a little expensive, $80/year is a lot. I use it maybe once or twice per month. I think you would have more customers if it was less expensive.
I couldnt have been happier with any other product!! This is awesome!
Easy to learn and use, lots of features that are helpful for my business
People Also Ask about form cms 1500
Is CMS 1500 paper or electronic?
The Form CMS-1500 is the standard paper claim form to bill Medicare Fee-For-Service (FFS) Contractors when a paper claim is allowed.
What is the difference between a UB 04 form and a CMS 1500 form?
The UB-04 (CMS-1450) form is the claim form for institutional facilities such as hospitals or outpatient facilities. This would include things like surgery, radiology, laboratory, or other facility services. The HCFA-1500 form (CMS-1500) is used to submit charges covered under Medicare Part B.
What is a CMS 1500 health insurance claim form?
The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers (DMERCs) when a provider qualifies for a waiver from the Administrative Simplification Compliance Act (ASCA) requirement for electronic submission of
Can you print CMS 1500 form?
You can preview and print CMS 1500 forms for claims associated with orders. CMS 1500 form printing is available only for orders with Claim Statuses other than No Insurance, No Claim, Billed to Patient, On Hold, or Void.
Can I print my own CMS 1500?
The only acceptable claim forms are those printed in Flint OCR Red, J6983, (or exact match) ink. Although a copy of the CMS-1500 form can be downloaded, copies of the form cannot be used for submission of claims, since your copy may not accurately replicate the scale and OCR color of the form.
Related pages
Related Content cms 1500 hcfa form
Related to cms 1500 hcfa form



Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.