Last updated on Mar 6, 2026

CMS L564/R297 2000 free printable template
pdfFiller is not affiliated with any government organization
Why choose pdfFiller for your legal forms?
All-in-one solution
pdfFiller offers a PDF editor, eSignatures, file sharing, collaboration tools, and secure storage—all in one place.
Easy to use
pdfFiller is simple, cloud-based, has a mobile app, and requires no downloads or a steep learning curve.
Secure and compliant
With encryption, user authentication, and certifications like HIPAA, SOC 2 Type II, and PCI DSS, pdfFiller keeps sensitive legal forms secure.
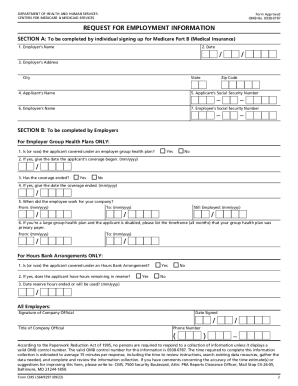
The Request for Employment Information is a government form used by the U.S. Department of Health and Human Services to collect employment and health coverage details from a claimant's employer.
pdfFiller scores top ratings on review platforms
Smooth, Easy
very valuable
unlike any other product on the market today
the forms are great and easy to fill out. Very user friendly. Unfortunately, I can't talk my boss into letting me keep it
I usually struggle to get documents either online, tax program, or fill out manually. PDF Filler has already made a difference and paid for itself
good
Who needs CMS L564R297?
Explore how professionals across industries use pdfFiller.

CMS L564R297 is needed by:
-
Employers verifying employee health coverage
-
Claimants needing health benefits
-
Government agencies processing benefit claims
-
Insurance companies assessing claims
-
Legal representatives handling employment disputes
What is the Request for Employment Information Form?
The Request for Employment Information Form is essential for the U.S. Department of Health and Human Services as it facilitates the collection of relevant employment and health coverage information for claimants. This form serves as a crucial document for employment verification and health coverage assessment, ensuring that accurate data is provided for processing claims.
This employment verification form is utilized by employers to confirm details about an employee’s work history, including their employment dates and the status of health coverage. By filling out this form, companies support individuals in securing necessary health benefits.
Purpose and Benefits of Completing the Request for Employment Information Form
Completing the Request for Employment Information Form is vital for both claimants and employers. Claimants can benefit greatly as accurate completion of this employment and health coverage form can assist in securing required health coverage. For employers, it is their responsibility to ensure that the information is filled out accurately, as this can affect the employee's eligibility for health plans.
Failure to provide correct information can lead to significant implications for health plan eligibility, potentially affecting the support available to claimants. Therefore, both parties have a vested interest in the correct completion of this form.
Who Needs to Complete the Request for Employment Information Form?
This form is typically required in various situations, especially concerning health insurance claims. Employers and company officials play critical roles in accurately completing and submitting the Request for Employment Information Form.
It’s important to clarify that eligibility for completing this form is contingent upon the individual's circumstances relating to health coverage and employment. Understanding these nuances ensures that the correct individuals request the form when necessary.
How to Fill Out the Request for Employment Information Form Online
Filling out the Request for Employment Information Form online can be straightforward with the right guidance. Begin by gathering the necessary information, which includes employment dates and health coverage status. To proceed, follow these steps:
-
Access the fillable form through a digital platform.
-
Enter the relevant employment details in the designated fields.
-
Provide the claimant's health coverage status and dates.
-
Ensure the form is signed and dated by a company official.
-
Include the necessary contact information for follow-up.
Highlighting the areas requiring official details is essential, as these will confirm the authenticity of the information provided.
Common Mistakes to Avoid When Filling Out the Form
When completing the Request for Employment Information Form, it is crucial to avoid common mistakes that could lead to delays or rejections. Common pitfalls include inaccuracies in entering employment dates and health coverage details. Ensure that:
-
All dates are double-checked for correctness.
-
Signatures and contact information are clearly included.
-
The form is thoroughly reviewed for any errors before submission.
Taking these precautions can help ensure a successful submission and minimize potential issues.
Submission Methods for the Request for Employment Information Form
Once completed, the Request for Employment Information Form can be submitted through several methods. Submitters have the option of mailing or electronically submitting the form. When opting for mailing, consider these best practices:
-
Use a secure envelope to protect personal information during transit.
-
Check for any required signatures before sending.
Confirming the receipt of your submission can often be managed using tools that allow for tracking, enhancing the assurance that your documentation has been received.
What Happens After You Submit the Request for Employment Information Form?
After the submission of the Request for Employment Information Form, claimants can expect a processing timeline based on the reviewing authority's schedule. It is advisable to track the status of the submission through established methods to ensure all documentation is in order.
If there are any issues with the submission, it is crucial to be aware of what actions can be taken to resolve potential problems. Knowing the common rejection reasons can help in preparing for possible follow-up actions.
The Role of pdfFiller in Completing the Request for Employment Information Form
pdfFiller plays a significant role in simplifying the process of completing the Request for Employment Information Form. Key features that assist users include:
-
Editable form fields to customize the document.
-
eSigning capabilities for secure and efficient authorization.
-
Security measures that protect sensitive information throughout the editing process.
By utilizing pdfFiller, users can experience a more efficient and stress-free completion process, making form management seamless.
Additional Resources and Support for Completing the Request for Employment Information Form
For users seeking further assistance, multiple additional resources are available. Access to downloadable templates or examples of completed forms can provide clarity on the form-filling process. Support options include:
-
Contact information for direct inquiries.
-
Links to relevant services that enhance the user experience through pdfFiller.
Exploring these resources can further aid in completing the form accurately and efficiently.
Get Started with the Request for Employment Information Form Today
Utilizing pdfFiller to complete the Request for Employment Information Form can streamline the process considerably. With a focus on correctly filling out this form, users are encouraged to leverage features provided for easy completion and signing. The user-friendly interface ensures that form management is accessible to everyone.
How to fill out the CMS L564R297
-
1.Begin by accessing the Request for Employment Information form on pdfFiller’s website. Use the search feature or browse the Government Forms section to locate the document. Open the form to start filling it out.
-
2.Once the form is open, utilize pdfFiller’s intuitive interface to navigate through the different fields. Click on each section to enter the requested information, ensuring you fill out each required field indicated on the form.
-
3.Before starting, gather all necessary details such as employment dates, health coverage status, and coverage dates. Ensure that you have the claimant's information at hand, as it's essential for providing accurate details.
-
4.Review the completed form carefully to check for any missing information or errors. Make sure all information is accurate and clearly legible. Double-check that you have filled out the sections that require the signature of a company official.
-
5.To finalize the form, use the options available on pdfFiller to save your progress. You can download a copy for your records or submit it electronically through the platform. Be sure to follow any specific submission guidelines provided.

Who needs to fill out the Request for Employment Information form?
The Request for Employment Information form must be filled out by the claimant's employer. They are responsible for providing accurate employment details and health coverage information to assist with the claimant's benefits process.
What supporting documents are required when submitting this form?
Typically, supporting documents such as employee records, health coverage confirmations, or any relevant identification may need to accompany this form. It's advisable to check with the requesting agency for specific requirements.
How is the Request for Employment Information form submitted?
You can submit the Request for Employment Information form electronically through pdfFiller or print it out and submit it by mail. Ensure you follow the specific submission instructions provided by the agency requesting the form.
Are there any deadlines for submitting this form?
While there may not be a strict deadline for submitting the Request for Employment Information, it is crucial to provide it promptly to avoid delays in the claimant's benefits processing. Check with the relevant agency for time-sensitive requirements.
What common mistakes should be avoided when completing this form?
Common mistakes include leaving required fields blank, providing inaccurate details, or forgetting to obtain the required signature. Always double-check the form before submitting to ensure completeness and accuracy.
What should I do if my employer is unable to fill out the form?
If your employer is unable to complete the Request for Employment Information form, you may reach out to an HR representative or a supervisor for assistance. If they are still unresponsive, consult the agency that requires the form for further advice.
How can I track the status of my Request for Employment Information form?
To track the status of your submitted Request for Employment Information form, contact the agency to which you submitted the form. They will provide you with information on the processing status and any further steps needed.
CMS L564/R297 Form Versions
Related Content
Related forms


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.