Get the free cms 1500 print text only
Show details
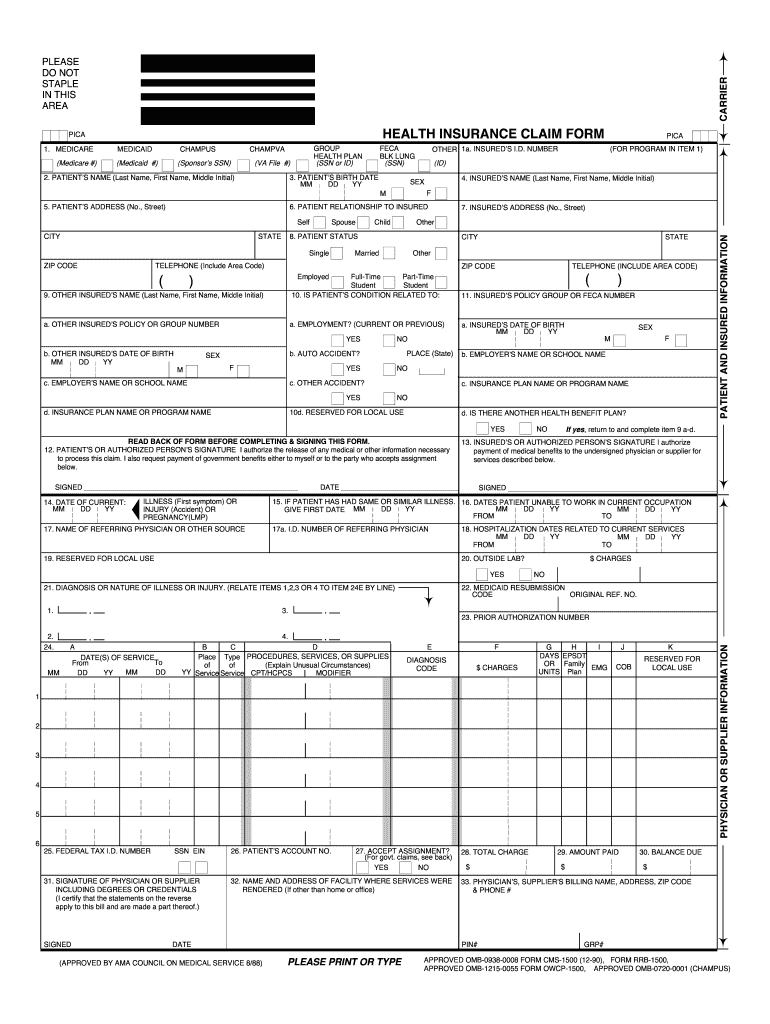
PICA 1. MEDICARE MEDICAID CAMPUS CHAM PVA HEALTH INSURANCE CLAIM FORM GROUP HEALTH PLAN (SSN or ID) DD BY FCA BULK LUNG (SSN) OTHER 1a. INSURED'S I.D. NUMBER PICA (FOR PROGRAM IN ITEM 1) (Medicare
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign fillable 1500 form
Edit your cms 1500 fillable form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your printable cms 1500 form pdf form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing printable cms 1500 form online



Use the instructions below to start using our professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit fillable cms 1500 claim form pdf. Text may be added and replaced, new objects can be included, pages can be rearranged, watermarks and page numbers can be added, and so on. When you're done editing, click Done and then go to the Documents tab to combine, divide, lock, or unlock the file.
4
Save your file. Select it from your records list. Then, click the right toolbar and select one of the various exporting options: save in numerous formats, download as PDF, email, or cloud.
The use of pdfFiller makes dealing with documents straightforward.
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
How to fill out cms 1500 form pdf
How to fill out blank CMS 1500 form:
01
Begin by entering your personal information in the appropriate fields. This includes your name, address, and contact details.
02
Next, provide the necessary details about the insured individual. This includes their name, date of birth, and insurance policy information.
03
In the "Patient's Relationship to Insured" field, indicate the relationship between the patient and the insured individual (e.g., self, spouse, child).
04
Proceed to enter the patient's information, which includes their name, date of birth, gender, and contact details.
05
Specify the patient's health insurance information, including their policy number, group number, and any other relevant details.
06
Indicate any prior authorization or referral numbers, if applicable.
07
Provide the dates of service for the medical procedures or treatments being claimed.
08
Enter the appropriate diagnosis and procedure codes for each service rendered. These codes should accurately reflect the medical services provided and should be consistent with the patient's medical records.
09
When listing the charges for each service, ensure that they correspond to the appropriate procedure codes.
10
Include any additional information that may be required, such as remarks or special instructions.
11
Double-check all the information entered for accuracy and completeness before submitting the form.
Who needs the blank CMS 1500 form:
01
Healthcare providers such as doctors, hospitals, and clinics use the CMS 1500 form to submit claims for reimbursement from health insurance companies.
02
Medical billing and coding professionals, as well as medical office staff, often handle the completion and submission of CMS 1500 forms on behalf of healthcare providers.
03
Patients who are uninsured but wish to submit a claim for medical services or seek reimbursement from their insurance company may also need the blank CMS 1500 form.
Fill
hcfa 1500 form pdf
: Try Risk Free
People Also Ask about 1500 pdf
What is the difference between CMS 1500 and UB 04 form?
The UB-04 (CMS-1450) form is the claim form for institutional facilities such as hospitals or outpatient facilities. This would include things like surgery, radiology, laboratory, or other facility services. The HCFA-1500 form (CMS-1500) is used to submit charges covered under Medicare Part B.
Why is it important to complete both UB-04 and CMS 1500 forms accurately?
It is critical to accurately complete both the UB-04 and CMS-1500 claim forms to ensure that healthcare providers receive timely and accurate reimbursement for the services they provide, as well as to avoid errors that can result in delays, denials, or incorrect payments.
How do I print a 1500 claim form?
To print text only on a blank, pre-existing CMS 1500 form: Navigate to the Claims module and select Claims Manager. Select the claims to be exported. Click the Actions. drop-down and select Export/Download. Select CMS 1500 (PDF) from the drop-down and click Export.
What is the difference between CMS and UB04?
The CMS-1450 form is printed with “red ink” on a standard white paper. The UB-04 is the electronic version of CMS-1450 only.
What is a OWCP 1500 form?
Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical Services Provided Under the FEDERAL EMPLOYEES' COMPENSATION ACT (FECA), the BLACK LUNG BENEFITS ACT (BLBA), and the ENERGY EMPLOYEES OCCUPATIONAL ILLNESS.
How do I get a CMS 1500 form?
In order to purchase claim forms, you should contact the U.S. Government Printing Office at 1-866-512-1800, local printing companies in your area, and/or office supply stores. Each of the vendors above sells the CMS-1500 claim form in its various configurations (single part, multi-part, continuous feed, laser, etc).
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
How do I edit 1500 medical form online?
pdfFiller not only allows you to edit the content of your files but fully rearrange them by changing the number and sequence of pages. Upload your cms 1500 pdf to the editor and make any required adjustments in a couple of clicks. The editor enables you to blackout, type, and erase text in PDFs, add images, sticky notes and text boxes, and much more.
How can I fill out hcfa 1500 pdf on an iOS device?
Install the pdfFiller iOS app. Log in or create an account to access the solution's editing features. Open your hcfa form pdf by uploading it from your device or online storage. After filling in all relevant fields and eSigning if required, you may save or distribute the document.
How do I complete imgurl pid 1 7 on an Android device?
Use the pdfFiller app for Android to finish your fillable hcfa 1500 form. The application lets you do all the things you need to do with documents, like add, edit, and remove text, sign, annotate, and more. There is nothing else you need except your smartphone and an internet connection to do this.
What is cms 1500 print text?
The CMS 1500 print text is a standardized claim form used by healthcare providers to bill for services rendered to patients and to request reimbursement from insurance carriers.
Who is required to file cms 1500 print text?
Healthcare providers such as physicians, therapists, and other professionals who provide medical services and wish to file claims with insurance companies are required to use the CMS 1500 print text.
How to fill out cms 1500 print text?
To fill out the CMS 1500 print text, providers must enter patient information, insurance details, services rendered, and billing codes in the designated fields of the form, ensuring accuracy and compliance with insurance guidelines.
What is the purpose of cms 1500 print text?
The purpose of the CMS 1500 print text is to facilitate the billing process by providing a standardized format for submitting medical claims to insurance companies, which helps ensure proper reimbursement for services.
What information must be reported on cms 1500 print text?
The CMS 1500 print text must report patient demographics, provider information, details of medical services provided, diagnosis codes, procedure codes, charges for services, and any applicable insurance information.
Fill out your cms 1500 print text online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Cms 1500 Printable Form is not the form you're looking for?Search for another form here.
Keywords relevant to cms 1500 form pdf fillable
Related to hcfa pdf



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
