Last updated on Apr 3, 2026
Get the free Medicaid Medication Appeal Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is medicaid medication appeal request
The Medicaid Medication Appeal Request Form is a healthcare document used by members or their representatives to appeal medication coverage decisions.
pdfFiller scores top ratings on review platforms
Who needs medicaid medication appeal request?
Explore how professionals across industries use pdfFiller.

Medicaid medication appeal request is needed by:
-
Medicaid recipients looking to appeal medication coverage decisions
-
Physicians assisting patients in the appeal process
-
Authorized representatives of members filing on behalf of others
-
Healthcare providers requiring a formal appeal for treatment
-
Social workers supporting clients navigating Medicaid processes
Comprehensive Guide to medicaid medication appeal request
What is the Medicaid Medication Appeal Request Form?
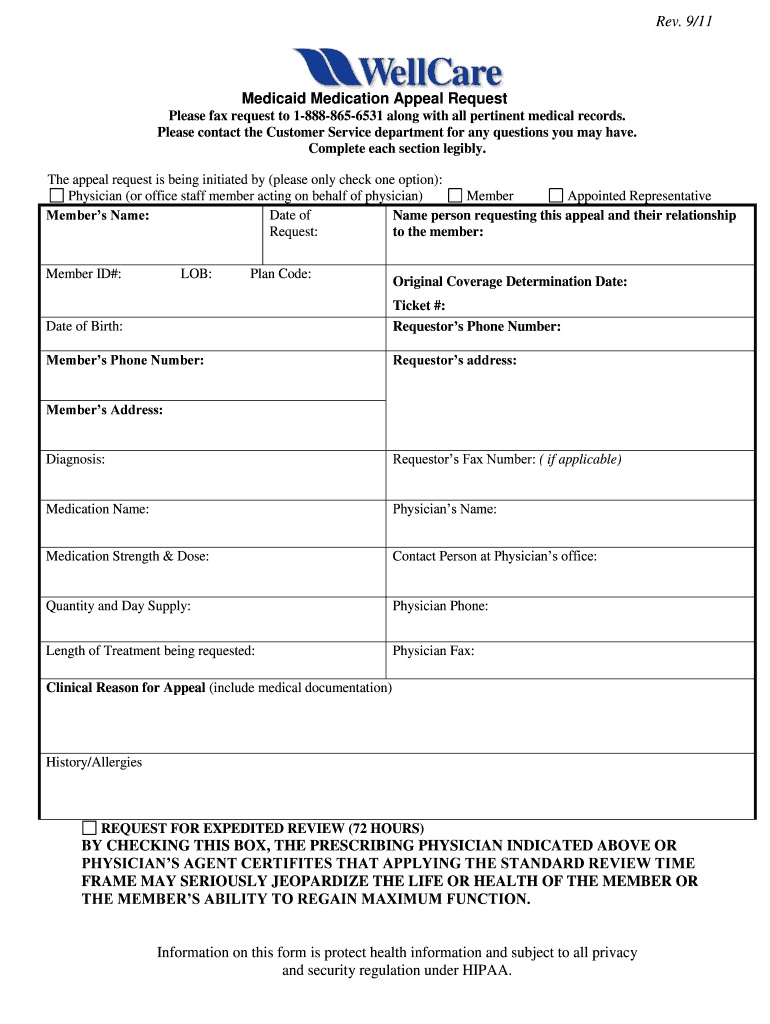
The Medicaid Medication Appeal Request Form is a vital document that allows members, physicians, and representatives to appeal decisions regarding medication coverage. This form is essential in ensuring that individuals have access to necessary treatments when their coverage is denied. Such appeals typically arise when a prescribed medication is deemed not medically necessary by the insurance provider.
Utilized by a range of stakeholders, including members and healthcare providers, the form serves as a formal request for reconsideration of medication coverage decisions. Situations that necessitate this form include instances when prescribed medications are denied or when there is a need for alternatives not covered by standard policies.
Purpose and Benefits of the Medicaid Medication Appeal Request Form
This form empowers members to challenge determinations made about their medication coverage. When members believe that a specific medication is necessary for their health and is unjustly denied, filling out the form initiates a formal appeal process. Among the benefits of using this form is the opportunity for members to secure access to necessary medications that can have a significant impact on their health outcomes.
Furthermore, in urgent cases where waiting for a standard review could jeopardize health, the form also allows for an expedited review process, ensuring that critical medications can be accessed promptly. This feature greatly enhances the overall effectiveness of the healthcare appeal process.
Key Features of the Medicaid Medication Appeal Request Form
The Medicaid Medication Appeal Request Form includes several essential fillable fields designed to gather pertinent information, such as Member Name, Member ID, Date of Birth, Medication Name, and Physician's Name. Additionally, the form features checkboxes that specify the types of requestors and allows users to articulate the clinical reasons behind the appeal.
One significant advantage of this form is its compatibility with pdfFiller, which promotes digital versatility. This enables users to easily edit and submit their forms online, improving the efficiency of the appeal process.
Who Needs the Medicaid Medication Appeal Request Form?
The Medicaid Medication Appeal Request Form is intended for various stakeholders, including Medicaid beneficiaries, healthcare providers, and authorized representatives who are assisting members with their appeals. Understanding who can legally submit the form is crucial, as it assures that the provided information is valid and the appeals process is properly initiated.
This form is particularly important in situations where denial of medication coverage must be formally contested, ensuring that rightful claims can be effectively reviewed and potentially reversed.
How to Fill Out the Medicaid Medication Appeal Request Form Online
Filling out the Medicaid Medication Appeal Request Form online using pdfFiller is straightforward. Users can follow these simple steps:
-
Access the form via pdfFiller’s platform.
-
Complete all required fillable fields accurately, including personal and medication details.
-
Utilize annotation tools to provide additional information or context for the appeal.
-
Review the completed form to ensure all information is correct and comprehensive.
-
Submit the form electronically through the platform.
It is vital to ensure that all information is accurately filled out, as omissions or mistakes may lead to delays in the review process.
Common Errors and How to Avoid Them
When completing the Medicaid Medication Appeal Request Form, certain common mistakes can hinder the appeal process. These may include incomplete fields, incorrect medication information, or failure to provide necessary clinical documentation. To prevent these issues, follow these actionable tips:
-
Double-check all entries for accuracy.
-
Ensure that all required fields are filled out completely.
-
Include detailed clinical reasons that support the appeal.
-
Validate that the physician’s information matches their credentials.
Thorough and precise documentation is critical in ensuring a smooth appeal process.
Submission Method of the Medicaid Medication Appeal Request Form
Once the Medicaid Medication Appeal Request Form has been completed, it is crucial to know how to submit it correctly. There are typically two methods of submission: online and physical. When submitting online through pdfFiller, users can follow straightforward electronic processes that streamline efficiency.
In cases where physical submission is necessary, ensure that the form is sent to the correct address and that any associated fees are understood, including potential fee waivers.
After Submission: What to Expect
Upon submission of the Medicaid Medication Appeal Request Form, members should be aware of the following steps in the process. Typically, there is a set processing time for appeals, and confirmation of receipt will be provided by the reviewing entity. Members may track the status of their appeal through designated channels, ensuring they remain informed about any updates or required actions.
Additionally, it's important to recognize that appeals can yield various outcomes, including approvals, denials, or requests for additional information to support the claim.
Ensuring Security and Compliance When Using the Medicaid Medication Appeal Request Form
Data protection is critical when handling sensitive information related to the Medicaid Medication Appeal Request Form. Compliance with regulations such as HIPAA and GDPR is essential for safeguarding patients’ privacy. pdfFiller ensures security through robust measures, including 256-bit encryption, which protects information against unauthorized access.
Using this service grants reassurance regarding the secure handling of appeals and the integrity of submitted documents, ensuring compliance with health regulations.
Experience the Ease of Filing with pdfFiller
To streamline the completion and submission of the Medicaid Medication Appeal Request Form, leverage the innovative tools available through pdfFiller. The platform offers user-friendly features that enhance the overall experience of filling out forms, making the process efficient and straightforward.
Explore how pdfFiller can facilitate healthcare documentation processes, simplifying the necessary tasks associated with appeals and making access to critical medications more attainable.
How to fill out the medicaid medication appeal request
-
1.To access the Medicaid Medication Appeal Request Form on pdfFiller, visit the pdfFiller website and log in to your account. If you don’t have an account, you can create one for free.
-
2.Once logged in, use the search bar to type 'Medicaid Medication Appeal Request Form' and select it from the results.
-
3.Begin filling out the form by clicking on the first fillable field for Member Name. Enter the name as it appears on your Medicaid card.
-
4.Continue to the Member ID field, where you should input the unique identifier associated with the member's Medicaid profile.
-
5.In the Date of Birth field, select the appropriate date from the calendar provided, ensuring it reflects the member’s birthdate.
-
6.Next, navigate to the Medication Name field. Clearly specify the name of the medication for which you are appealing coverage.
-
7.Provide the Physician's Name by filling in the name of the healthcare provider prescribing the medication. This can help with the appeal review process.
-
8.If applicable, check the boxes indicating the type of requestor, whether the member, a physician, or an authorized representative is submitting the form.
-
9.In the clinical reasons section, describe the justification for the appeal in detail. Use clear and concise language to articulate why the medication is necessary.
-
10.Once all fields are filled, review the entire form to ensure that all information is accurate and complete. Look for any missed fields indicated by pdfFiller’s prompts.
-
11.After reviewing, finalize the form. Use the save option to store your completed document in your pdfFiller account securely.
-
12.You can download a copy of the form for your records or submit it directly to the relevant Medicaid office via the submit function on pdfFiller.

Who is eligible to submit the Medicaid Medication Appeal Request Form?
Any Medicaid recipient, their authorized representative, or a physician can submit this form to appeal medication coverage decisions.
Are there deadlines for submitting the appeal form?
Yes, it's important to submit the Medicaid Medication Appeal Request Form as soon as possible after receiving a denial to ensure timely processing.
How should I submit the completed appeal form?
You can submit the Medicaid Medication Appeal Request Form electronically through pdfFiller or print and mail it to the designated Medicaid office.
What supporting documents are needed with the form?
Typically, you may need to include a prescription or letter from the physician detailing the medication's necessity to support your appeal.
What common mistakes should I avoid when filling out this form?
Avoid incomplete fields, unclear explanations, and ensure that all required signatures and contact information are included before submitting the form.
How long does it take to process the appeal once submitted?
The processing time for appeals can vary; however, expect a decision within 30 days after submission, or sooner if an expedited review is requested.
Is notarizing the Medicaid Medication Appeal Request Form necessary?
No, notarization is not required for the Medicaid Medication Appeal Request Form, making it more accessible for users.
Related Forms





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.