Add or replace text, adjust formatting, insert legally binding eSignatures, and send documents for signing without hopping between apps.
EleCare Template Letter of Medical Necessity 2012 free printable template
Show details
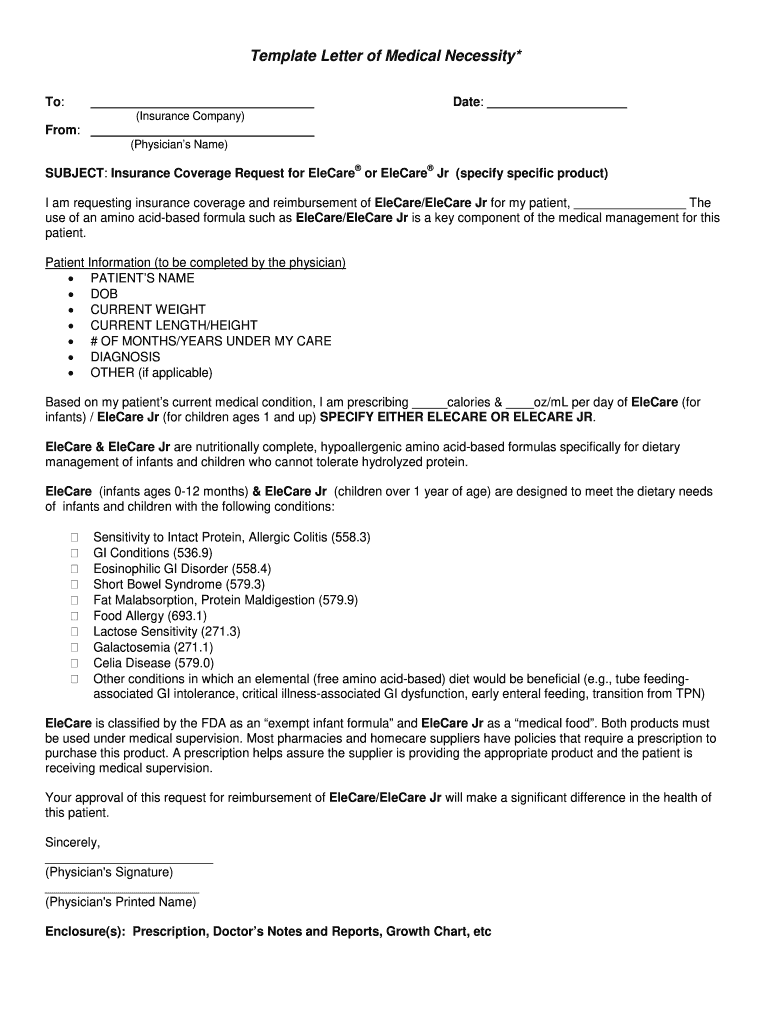
Template Letter of Medical Necessity* To: Date: (Insurance Company) From: (Physician s Name) SUBJECT: Insurance Coverage Request for Elevate or Elevate Jr (specify specific product) I am requesting
pdfFiller is not affiliated with any government organization
Fill out, sign, and share forms from a single PDF platform
Manage all your documents quickly and securely in the cloud.
Edit and sign in one place
Create professional forms
Add and customize fillable fields to tailor each form to your needs and ensure easy completion without printing and scanning.
Simplify data collection
Quickly share forms via email or a secure link, enabling anyone to complete forms online in seconds, on any device.
Manage forms centrally
Keep all your forms and templates organized in one secure, cloud-based platform, track changes easily, and export documents in any format.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
Understanding the EleCare Template Letter of Form
What is the EleCare Template Letter of Form?
The EleCare template letter of form serves as a structured document used by healthcare providers to request insurance coverage for EleCare or EleCare Jr, specialized nutritional products for patients with specific medical needs. This form is vital for demonstrating the medical necessity of these amino acid-based formulas, which are essential for patients who cannot tolerate standard protein sources.
Key Features of the EleCare Template Letter of Form
This form outlines essential patient information like name, date of birth, and specific medical diagnoses that necessitate the use of EleCare products. It includes prescribed dosages and details on the medical conditions related to the patient’s digestive health, providing a comprehensive overview to insurance companies.
Eligibility Criteria for the EleCare Template Letter of Form
To successfully utilize the EleCare template letter of form, patients typically must meet specific eligibility criteria defined by their insurance provider. Generally, this includes a diagnosis that justifies the medical necessity of an elemental diet, alongside physician confirmation of the patient’s ongoing healthcare needs.
Required Documents and Information
When filling out the EleCare template letter of form, providers need to ensure they have all pertinent information. This includes the patient’s medical history, specific dietary needs, and any previous medication or treatment plans that support the request for EleCare or EleCare Jr. Proper documentation is key for validation by insurance companies.
How to Fill the EleCare Template Letter of Form
Filling out the EleCare template letter requires careful attention to detail. Start by inputting the patient’s information accurately, ensuring all medical conditions and prescribed dosages are clearly stated. It is critical to articulate the necessity of the product in treating the patient's conditions, supported by any relevant clinical evidence.
Common Errors and Troubleshooting
Common mistakes may include incomplete patient information, lack of supporting documentation, or unclear medical necessity statements. Providers should review the form carefully before submission, ensuring all fields are filled out correctly and extra documentation is attached as needed to avoid delays in insurance processing.
Frequently Asked Questions about sample letter of medical necessity for hot tub form
What is the purpose of the EleCare template letter of form?
The purpose is to formally request insurance coverage for EleCare or EleCare Jr by outlining the medical necessity for these nutritional formulas based on the patient's health condition.
pdfFiller scores top ratings on review platforms
Amazing product! I was able to fill a tax form very easily and sign it. Better than all others I've tried!
There are two comments for the development team and marketing team: 1/I expected a free trial, and 2/There are so many options that it can be confusing when you are just starting. I would have appreciated less options up front and some video tutorials to introduce me to advanced features.
I have found it easy to navigate and it gives a professional finish to documents
People Also Ask about letter of medical necessity
What is the criteria to determine medical necessity?
Medical necessity refers to a decision by your health plan that your treatment, test, or procedure is necessary to maintain or restore your health or to treat a diagnosed medical problem. In order to be covered under the health plan, a service must be considered medically necessary.
How do you prove medical necessity?
How is “medical necessity” determined? A doctor's attestation that a service is medically necessary is an important consideration. Your doctor or other provider may be asked to provide a “Letter of Medical Necessity” to your health plan as part of a “certification” or “utilization review” process.
What is an example of medical necessity?
"Medically Necessary" or "Medical Necessity" means health care services that a physician, exercising prudent clinical judgment, would provide to a patient. The service must be: For the purpose of evaluating, diagnosing, or treating an illness, injury, disease, or its symptoms.
What is an example of a letter of medical necessity for medication?
Dear [Insert Contact Name]: [Insert Patient Name] has been under my care for [Insert Diagnosis] [Insert ICD-10-CM Code] since [Insert Date]. Treatment of [Insert Patient Name] with [medication] is medically appropriate and necessary and should be covered and reimbursed.
How do I get a letter of medical necessity from my doctor?
A patient can write the letter, but it needs to be made official by a doctor. Any arguments for any service ultimately have to come from a treating physician. That means the doctor needs to know you, have some history with you, and in the end either write or 'sign off on' the letter.
What should a letter of medical necessity include?
A letter of medical necessity is typically written by your healthcare provider and includes your diagnosis and duration of the treatment. It should also include the reason why the treatment, product, or service is needed. A letter of medical necessity does not guarantee that your expense will be approved.
What are statements of medical necessity?
A letter of medical necessity (LOMN) is a document from your licensed healthcare provider that recommends a particular treatment, product, or equipment for medical purposes. The letter often includes relevant patient history, medical needs, and the duration of the treatment.
What is an example of a medical necessity statement?
The [PATIENT NAME] has a diagnosis of [DIAGNOSIS] and needs treatment with [INSERT PRODUCT], and that [INSERT PRODUCT] is medically necessary for [him/her] as prescribed. On behalf of the patient, I am requesting approval for use and subsequent payment for the [TREATMENT].
Related pages
Related Content letter of medical necessity
Related to letter of medical necessity






Related Catalogs
If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.