Last updated on May 14, 2026
CMS L564/R297 2016 free printable template
pdfFiller is not affiliated with any government organization

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
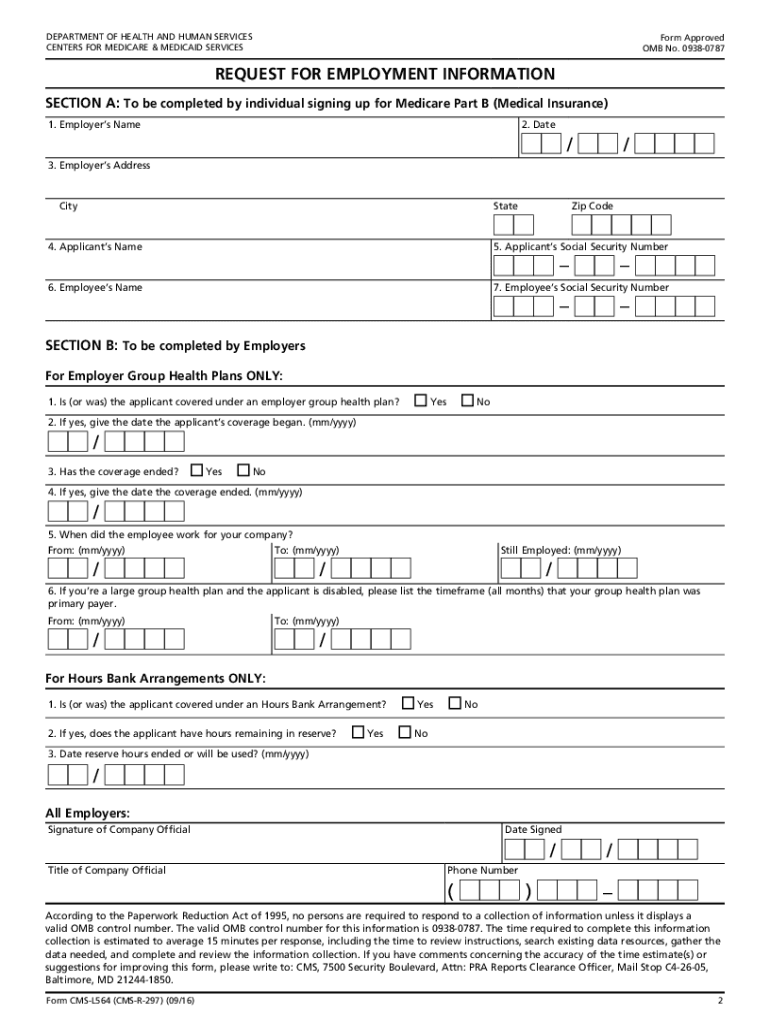
What is CMS L564/R297
The Request for Employment Information form (CMS-L564) is a government document used by Medicare applicants to verify group health plan coverage based on employment.
pdfFiller scores top ratings on review platforms
Smooth, Easy
very valuable
unlike any other product on the market today
the forms are great and easy to fill out. Very user friendly. Unfortunately, I can't talk my boss into letting me keep it
I usually struggle to get documents either online, tax program, or fill out manually. PDF Filler has already made a difference and paid for itself
good
Who needs CMS L564/R297?
Explore how professionals across industries use pdfFiller.

CMS L564/R297 is needed by:
-
Medicare applicants seeking coverage verification
-
Employers providing health insurance information
-
Social Security offices processing Medicare applications
-
Health insurance providers verifying employee coverage
-
Regulatory agencies requiring employment verification
Comprehensive Guide to CMS L564/R297
What is the Request for Employment Information?
The Request for Employment Information form, known as CMS-L564, is pivotal for verifying group health plan coverage in relation to Medicare enrollment. This form serves as crucial documentation in the Medicare Part B application process, ensuring that applicants can substantiate their current or past employment status. Essential details required in this form include the applicant’s Social Security number, employment dates, and employer information, which directly impact the enrollment process.
Purpose and Benefits of the Request for Employment Information
The Request for Employment Information form plays a significant role in confirming eligibility for Medicare by verifying group health plan coverage. For companies, utilizing this form streamlines the process of confirming employee health coverage and ensures compliance with Medicare requirements. Timely and accurate submission of the form is vital for Medicare Part B enrollment, minimizing potential delays and complications in accessing necessary healthcare services.
Who Needs the Request for Employment Information?
Primary users of the Request for Employment Information include both applicants seeking Medicare enrollment and company officials responsible for providing accurate employment verification. The form is especially crucial in scenarios such as new applicants entering the Medicare system and individuals experiencing job changes or transitions in health coverage. Various types of coverage, including employer-sponsored health plans, necessitate this verification to facilitate a smooth enrollment process.
Key Features of the Request for Employment Information Form
The CMS-L564 form contains several key sections and fillable fields. These sections require specific information from the applicant and the employer, including employment status and coverage details. The applicant must complete the initial section, while the employer fills out the subsequent part and provides a signature. Notarization is generally not required, but both roles must ensure accurate and complete information to avoid issues during submission.
How to Fill Out the Request for Employment Information Online (Step-by-Step)
-
Access the CMS-L564 form via pdfFiller’s platform.
-
Begin by entering your personal information, including your Social Security number.
-
Have your employer complete their portion of the form with relevant employment details.
-
Ensure both parties check all fields for accuracy before signing.
-
Submit the completed form as directed using your preferred submission method.
To avoid common errors, carefully review the form for completeness and accuracy, ensuring all required fields are filled correctly. Utilize tools on pdfFiller to help with guided completion.
Submission Methods for the Request for Employment Information
There are several methods available for submitting the Request for Employment Information form. Applicants can choose to submit the form online via pdfFiller, through traditional mail, or in person at their local Social Security office. Each submission method has specific guidelines and timelines; therefore, tracking the submission can help ensure the timely processing of Medicare applications.
Security and Compliance for the Request for Employment Information
When handling personal information through the Request for Employment Information form, security is paramount. pdfFiller adheres to stringent compliance standards, including HIPAA and GDPR, ensuring that all user data is protected. To enhance the security of your submission, always use secure networks and verify the authenticity of the submission methods being utilized.
Common Errors and How to Avoid Them
-
Leaving fields incomplete or mislabeling information.
-
Failing to secure necessary signatures from both the applicant and employer.
-
Submitting outdated forms that do not reflect current enrollment criteria.
-
Neglecting to double-check Social Security numbers and other critical details.
To minimize errors, create a checklist that reviews all required documents and verify every section before the final submission. This practice will enhance the likelihood of a successful Medicare enrollment process.
Sample or Example of a Completed Request for Employment Information
To facilitate understanding, a visually formatted example of a completed Request for Employment Information is provided. Each section is clearly labeled to illustrate what constitutes accurate submissions. Key takeaways from this example include the necessity of completeness in all sections and ensuring all parties have adhered to signing requirements for the form to be valid.
Getting Started with pdfFiller to Complete Your Form
Utilizing pdfFiller's tools can significantly streamline the process of completing the Request for Employment Information form. The platform offers user-friendly features for document management and eSigning, ensuring both ease and security in handling personal information. Additional resources are available within pdfFiller to assist users in navigating the submission process effectively.
How to fill out the CMS L564/R297
-
1.Access the Request for Employment Information form by searching for it on pdfFiller. Use the search bar or browse government forms until you find CMS-L564.
-
2.Open the form in pdfFiller. Once loaded, familiarize yourself with the layout and navigation tools available on the platform.
-
3.Before beginning, gather necessary information such as your Social Security number, employer details, and employment dates.
-
4.Start filling in the first section of the form, which requires your personal information including your full name and date of birth. Use the fillable fields to type your details.
-
5.Next, move to the employer's section. Here, the employer should input their contact information and sign the document. They can also add any additional data if required.
-
6.Ensure that all fields are completed properly, checking for any missing information or errors that may need correction.
-
7.Once all sections are filled, review the entire document for accuracy. Confirm that both the applicant and the employer have provided their signatures.
-
8.After final checks, save the document on pdfFiller. You can choose to download it or send it directly to the designated Social Security office for processing.

Who is eligible to use the Request for Employment Information form?
The form can be utilized by individuals applying for Medicare who need to verify their group health plan coverage based on their current or past employment.
What details must be included on the form?
You must provide your Social Security number, employment dates, and information regarding your employer's health insurance policy.
How do I submit the completed form?
The completed form should be submitted to your local Social Security office along with your Medicare Part B application. Check the office's website for specific submission guidelines.
Are there any deadlines for submitting the Request for Employment Information form?
It’s advisable to submit this form as soon as you apply for Medicare to avoid delays in coverage processing. Check with Medicare for specific deadlines related to your enrollment period.
What supporting documents are needed when submitting this form?
While completing the Request for Employment Information form, additional supporting documents may include proof of employment, your Medicare application, and any prior health coverage documents.
How long does it take to process the Request for Employment Information form?
Processing times can vary based on the Social Security office and the volume of applications received. Generally, allow several weeks for processing.
What common mistakes should I avoid on this form?
Make sure not to leave any required fields blank and double-check the accuracy of the information provided, especially your Social Security number and signatures from both parties.
CMS L564/R297 Form Versions
Related Content
Related Forms
Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.