OH ODM 06723 2017-2026 free printable template
Show details
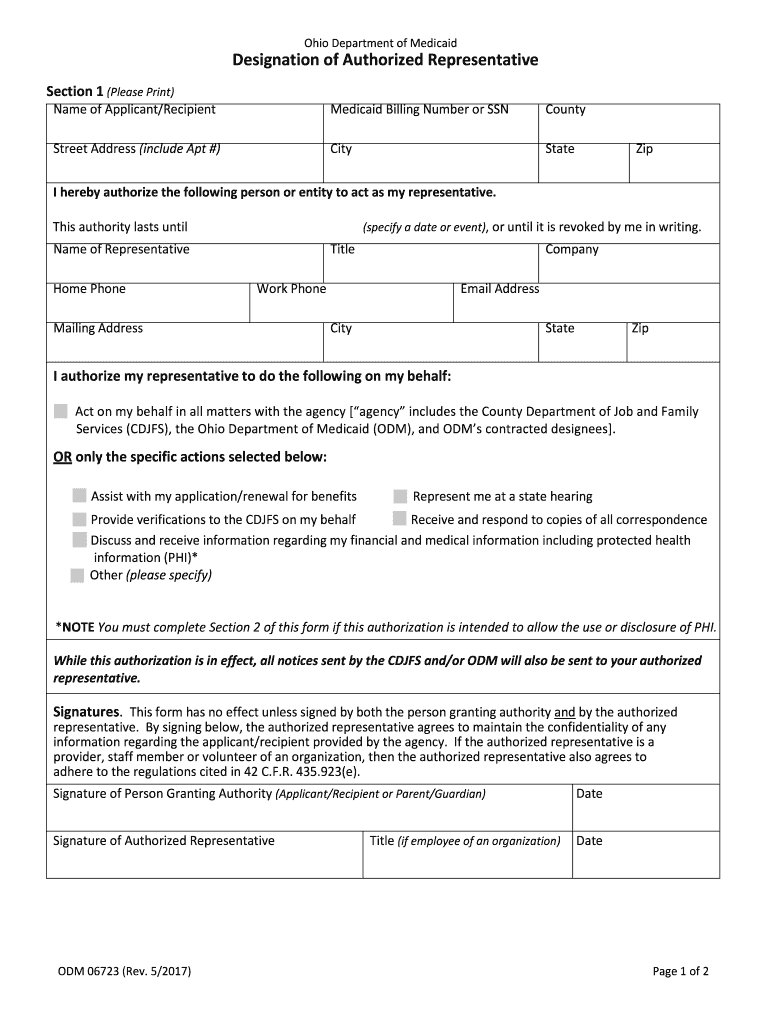
F.R. 435. 923 e. Signature of Person Granting Authority Applicant/Recipient or Parent/Guardian Date Signature of Authorized Representative ODM 06723 Rev. 5/2017 Title if employee of an organization Page 1 of 2 Section 2 Authorization for the Use and Disclosure of Protected Health Information Address Case Number/Medicaid ID Date of Birth Zip Code The County Department of Job and Family Services CDJFS the Ohio Department of Medicaid ODM and ODM s contracted designees including Medicaid managed...
pdfFiller is not affiliated with any government organization
Get, Create, Make and Sign odm 06723 form
Edit your medicaid authorized representative form form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your ohio medicaid authorized representative form form via URL. You can also download, print, or export forms to your preferred cloud storage service.
Editing authorized representative designation form online



To use the services of a skilled PDF editor, follow these steps:
1
Create an account. Begin by choosing Start Free Trial and, if you are a new user, establish a profile.
2
Simply add a document. Select Add New from your Dashboard and import a file into the system by uploading it from your device or importing it via the cloud, online, or internal mail. Then click Begin editing.
3
Edit designation of authorized representative form. Rearrange and rotate pages, insert new and alter existing texts, add new objects, and take advantage of other helpful tools. Click Done to apply changes and return to your Dashboard. Go to the Documents tab to access merging, splitting, locking, or unlocking functions.
4
Get your file. Select the name of your file in the docs list and choose your preferred exporting method. You can download it as a PDF, save it in another format, send it by email, or transfer it to the cloud.
pdfFiller makes working with documents easier than you could ever imagine. Create an account to find out for yourself how it works!
Uncompromising security for your PDF editing and eSignature needs
Your private information is safe with pdfFiller. We employ end-to-end encryption, secure cloud storage, and advanced access control to protect your documents and maintain regulatory compliance.
OH ODM 06723 Form Versions
Version
Form Popularity
Fillable & printabley
How to fill out how do i edit oh reported on oh odm 06723 form
How to fill out OH ODM 06723
01
Obtain the OH ODM 06723 form from the relevant authority's website or office.
02
Fill in the personal details section with accurate information such as name, address, and contact number.
03
Provide specific information regarding the purpose of the form, as required in the designated sections.
04
Attach any necessary documentation or proof that is required to support the information provided.
05
Review the completed form for any errors or missing information.
06
Sign and date the form where indicated.
07
Submit the form to the appropriate office or online portal as specified in the instructions.
Who needs OH ODM 06723?
01
Individuals applying for certain health benefits or services.
02
Healthcare providers submitting claims or requests for authorization.
03
Organizations that need to gather data for health services programs.
Fill
authorized representative form
: Try Risk Free
People Also Ask about authorized rep form medicaid
How do I get a refund from Medicaid in Ohio?
If the claim is within 3 years of the paid date, submit an adjustment request through the Electronic Data Interchange (EDI) or MITS web portal. If the claim is greater than 3 years and less than 7 years from the paid date, the adjustment can be submitted via the EDI adjustment process.
How do I contact Medicaid in Ohio?
We are here to help! Consumer Hotline 800-324-8680.
What is the timely filing limit for Ohio Medicaid?
(a) Three hundred sixty-five days of the actual date the service was provided.
How do I get a copy of my Ohio Medicaid card?
If you're an Ohio Medicaid member, call our Consumer Hotline at 800-324-8680. Otherwise, follow the links below for additional resources, or complete the Contact Us Form and we'll get back to you. Where is my card? We are here to help!
How do I cancel my Medicaid benefits in Ohio?
Call the Ohio Medicaid Hotline at 1-800-324-8680, Monday through Friday from 7 a.m. to 8 p.m., and Saturday from 8 a.m. to 5 p.m. TTY users should call the Ohio Relay Service at 7-1-1.
What is the designation of authorized representative?
A designated authorized representative agrees to act responsibly on behalf of the applicant/recipient by providing all necessary information to determine eligibility for assistance.
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
Can I create an eSignature for the odjfs authorized representative form in Gmail?
With pdfFiller's add-on, you may upload, type, or draw a signature in Gmail. You can eSign your authorized representative designation and other papers directly in your mailbox with pdfFiller. To preserve signed papers and your personal signatures, create an account.
How do I complete designation of authorized representative on an iOS device?
Install the pdfFiller app on your iOS device to fill out papers. Create an account or log in if you already have one. After registering, upload your ohio medicaid prior authorization form. You may now use pdfFiller's advanced features like adding fillable fields and eSigning documents from any device, anywhere.
How do I edit odm forms on an Android device?
You can. With the pdfFiller Android app, you can edit, sign, and distribute medicaid authorized representative form pdf from anywhere with an internet connection. Take use of the app's mobile capabilities.
What is OH ODM 06723?
OH ODM 06723 is a reporting form used by the Ohio Department of Medicaid to collect information regarding the eligibility and enrollment of individuals receiving Medicaid benefits.
Who is required to file OH ODM 06723?
Providers who offer Medicaid services or have any interaction with Medicaid beneficiaries are required to file OH ODM 06723 to ensure compliance with reporting requirements.
How to fill out OH ODM 06723?
To fill out OH ODM 06723, individuals must provide accurate personal and financial information as required by the form, including details about Medicaid eligibility, service types, and any changes in status.
What is the purpose of OH ODM 06723?
The purpose of OH ODM 06723 is to collect necessary data for the administration of Medicaid programs, help evaluate beneficiary eligibility, and ensure that services are provided in accordance with state and federal regulations.
What information must be reported on OH ODM 06723?
Information that must be reported on OH ODM 06723 includes personal identifiers, income details, household size, type of services rendered, and any changes that might affect eligibility for Medicaid.
Fill out your OH ODM 06723 online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Authorized Representative is not the form you're looking for?Search for another form here.
Keywords relevant to authorized representative form medicaid
Related to authorized representative request form





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.
