Last updated on Nov 22, 2017
Get the free Patient Application for Financial Assistance
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
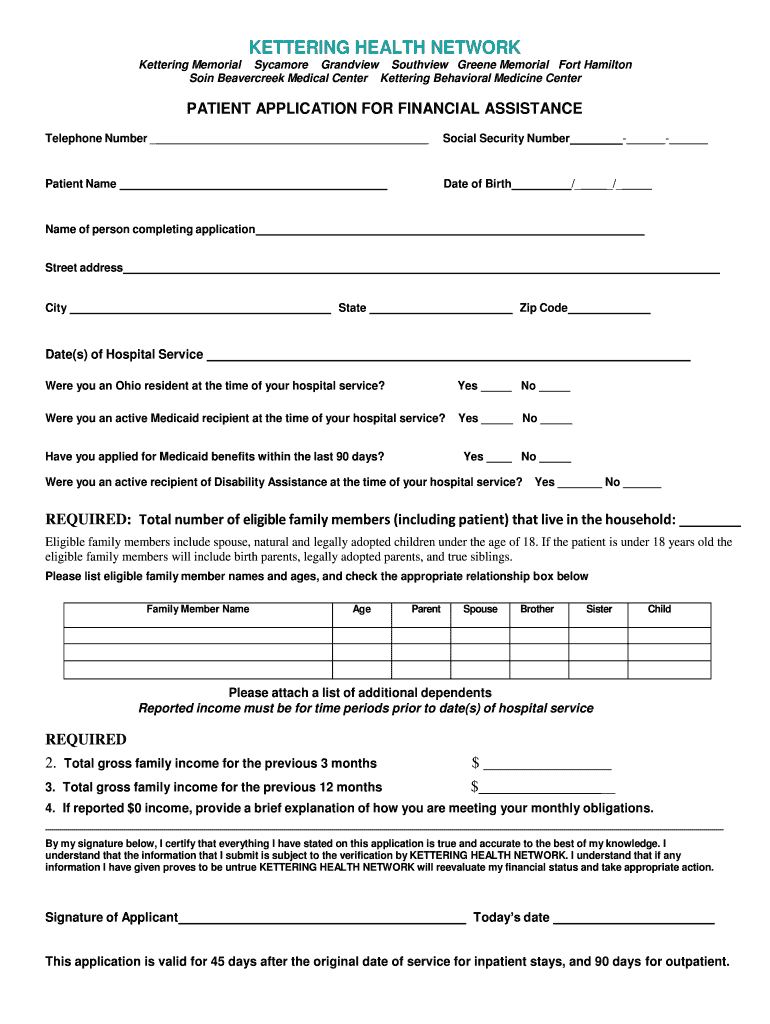
What is Financial Assistance Application
The Patient Application for Financial Assistance is a healthcare form used by individuals to apply for financial aid for hospital services at Kettering Health Network facilities in Ohio.
pdfFiller scores top ratings on review platforms
Who needs Financial Assistance Application?
Explore how professionals across industries use pdfFiller.

Financial Assistance Application is needed by:
-
Patients requiring financial assistance for healthcare services
-
Individuals seeking to support their medical costs at Kettering Health Network
-
Ohio residents needing aid for hospital bills
-
Families managing medical expenses for a member
-
Low-income individuals applying for financial support
-
Applicants eligible for Medicaid or Disability Assistance
Comprehensive Guide to Financial Assistance Application
What is the Patient Application for Financial Assistance?
The Patient Application for Financial Assistance is a crucial resource designed to help individuals secure financial aid for medical services at Kettering Health Network facilities in Ohio. This form serves as a means for patients to request for financial assistance, addressing potential barriers created by costs associated with their medical needs. It is important to be aware that the application is valid for specific time frames: 45 days for inpatient services and 90 days for outpatient services.
Purpose and Benefits of the Patient Application for Financial Assistance
The purpose of the Patient Application for Financial Assistance extends beyond merely filling out a form; it provides critical support for patients by alleviating financial burdens associated with medical care. By submitting this application, patients may become eligible for financial aid, which can significantly impact their ability to access necessary healthcare services at Kettering Health Network. The benefits of using this application include a clearer pathway to financial assistance and peace of mind during medical crises.
Who Needs to Complete the Patient Application for Financial Assistance?
This application is intended for a wide range of individuals who find themselves in challenging financial situations. Specifically, those who are low-income, uninsured, or underinsured may qualify for assistance. Key groups that may benefit from this application include families confronting medical emergencies or individuals needing extensive healthcare services. Understanding the target audience ensures that those who genuinely need support have access to this essential resource.
Eligibility Criteria for the Patient Application for Financial Assistance
To successfully complete the Patient Application for Financial Assistance, applicants must meet certain eligibility criteria. Primarily, this involves residency status, income guidelines, and considerations regarding Medicaid or Disability Assistance eligibility. Applicants should gather the required documentation, which typically includes proof of financial need, such as recent pay stubs, tax returns, and other relevant financial information.
How to Fill Out the Patient Application for Financial Assistance Online
Filling out the Patient Application for Financial Assistance online is straightforward when following these steps:
-
Access the application on the pdfFiller platform.
-
Enter personal information, such as your name and date of birth.
-
Provide family details, including income sources and members.
-
Make sure to complete all required fields accurately.
-
Review your application for errors before submission.
Common mistakes to avoid include leaving fields blank or providing incorrect information, as these errors can delay the application process.
Common Errors and How to Avoid Them in the Patient Application for Financial Assistance
When completing the Patient Application for Financial Assistance, being aware of common errors can enhance the likelihood of a successful submission. Typical pitfalls include:
-
Missing required fields, which can render the application incomplete.
-
Submitting incorrect or outdated personal information.
To avoid these issues, it is advisable to double-check all entries and ensure that documentation is current and relevant before submission.
Next Steps After Submitting the Patient Application for Financial Assistance
Once the Patient Application for Financial Assistance has been submitted, applicants can expect a review process. The timeline for decision-making regarding financial assistance may vary based on several factors. It is beneficial for applicants to track the application status and follow up with the financial assistance office if no response is received within the anticipated timeframe.
Privacy and Security When Using the Patient Application for Financial Assistance
Applying for financial assistance involves sharing sensitive information, making privacy and security paramount. pdfFiller implements robust security measures, including 256-bit encryption, to protect user data. The platform adheres to HIPAA and GDPR compliance standards, ensuring that all submitted documents maintain confidentiality and protection throughout the application process.
How pdfFiller Can Help You with the Patient Application for Financial Assistance
Using pdfFiller to complete the Patient Application for Financial Assistance offers numerous advantages. The platform simplifies the process of filling, editing, and eSigning the application. With its user-friendly interface, applicants can conveniently manage their documents online, making the completion and submission process more efficient.
Real-Life Example: Sample Completed Patient Application for Financial Assistance
To provide clarity, consider a mock-up of a completed Patient Application for Financial Assistance. This example includes annotations that explain each section, serving as a practical reference to assist users in visualizing how to accurately fill out the form. By reviewing a sample, applicants can better understand the information required and how to present it effectively.
How to fill out the Financial Assistance Application
-
1.Access the Patient Application for Financial Assistance form on pdfFiller by searching for its name or visiting the designated page.
-
2.Open the form, allowing you to view all necessary fields that require completion. Refer to the form's instructions while navigating.
-
3.Before completing the form, gather essential documents such as your Social Security Number, information regarding hospital services, and details about your family income.
-
4.Begin filling in the fields by inputting your personal information, including patient name, date of birth, and residency status. Use the interactive checkboxes for applicable questions.
-
5.Ensure all mandatory fields are completed, especially those requesting specifics about Medicaid and Disability Assistance status.
-
6.Continue filling out family member information and income details accurately to provide a clear financial picture.
-
7.Review the filled-out form closely for any errors or missing information. Utilize pdfFiller to check all fields are correctly filled before finalizing.
-
8.Once satisfied with the completed form, use pdfFiller’s options to save it to your devices or submit it directly to Kettering Health Network according to submission guidelines.

Who is eligible to apply for financial assistance?
Eligibility for financial assistance is typically defined by the patient's income level, residency in Ohio, and the specific services used at Kettering Health Network. Individuals facing financial hardship are encouraged to apply.
What is the submission deadline for the form?
The Patient Application for Financial Assistance must be submitted within a valid timeframe of 45 days for inpatient stays and 90 days for outpatient services. It is advisable to complete the form promptly.
How can I submit the completed form?
Completed applications can be submitted directly to Kettering Health Network facilities. You may follow instructions on pdfFiller to submit electronically or print and send it via mail.
What supporting documents do I need to include?
Supportive documents may include proof of income, residency status, and any details related to Medicaid or Disability Assistance applications. Check the specific requirements outlined in the form.
What are common mistakes to avoid when filling out the form?
Common mistakes include missing required fields, incorrect personal information, and failing to provide supporting documents. Double-check all entries before submitting.
What is the processing time for the financial assistance application?
Processing times for financial assistance applications may vary, but applicants should allow a few weeks for a response. It is also advisable to follow up with Kettering Health Network regarding your application status.
Is notarization required for this form?
No, notarization is not required for the Patient Application for Financial Assistance. However, a signature from the applicant is mandatory to validate the application.
Related Forms







Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.