Last updated on Apr 5, 2026
Get the free Patient Medical History Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is patient medical history form
The Patient Medical History Form is a healthcare document used by patients and guardians to provide comprehensive medical information to healthcare providers.
pdfFiller scores top ratings on review platforms
Who needs patient medical history form?
Explore how professionals across industries use pdfFiller.

Patient medical history form is needed by:
-
Patients seeking medical treatment
-
Guardians of minor patients
-
Healthcare providers conducting intake assessments
-
Medical offices requiring patient information
-
Insurance companies verifying patient health history
-
Hospitals ensuring complete pre-treatment data
-
Clinical researchers collecting health data for studies
Comprehensive Guide to patient medical history form
What is the Patient Medical History Form?
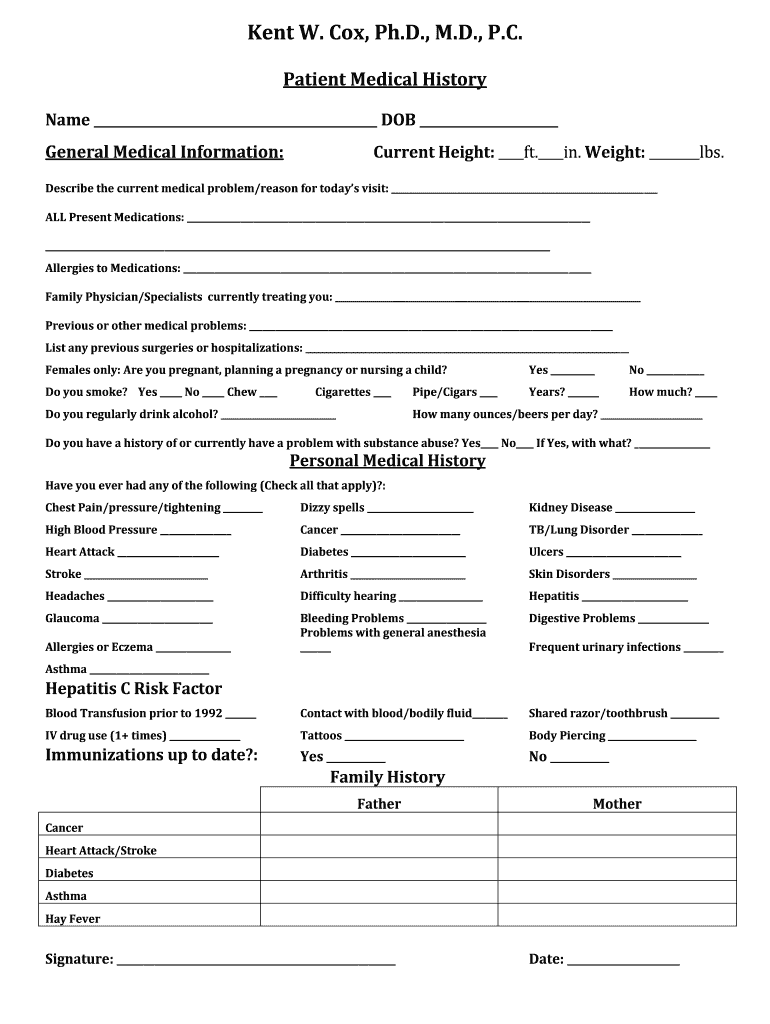
The Patient Medical History Form is an essential document used by healthcare providers to collect comprehensive medical information from patients. This healthcare intake form is crucial during initial visits and regular check-ups. It typically requires signatures from both patients and guardians for minors to ensure that all medical history is thoroughly documented. Features of this form include various sections that capture vital health details.
Purpose and Benefits of the Patient Medical History Form
The primary purpose of the Patient Medical History Form is to ensure that healthcare providers have accurate and complete medical histories for effective treatment. This health history questionnaire helps identify potential health risks, particularly through the family medical history section. It also enhances communication between patients and healthcare providers, promoting a deeper understanding of individual health needs.
Key Features of the Patient Medical History Form
The Patient Medical History Form is structured with essential features that facilitate easy completion. Users can expect the following:
-
Sections dedicated to general medical information, medications, and allergies.
-
Fillable fields that allow for easy input of information.
-
Checkboxes for quick yes/no responses.
-
Signature lines for necessary approvals.
-
Integration with digital tools for easy form completion.
Who Needs the Patient Medical History Form?
This form is particularly relevant for various groups:
-
Patients visiting healthcare providers for the first time.
-
Guardians completing forms for minor patients.
-
Individuals seeking care from different specializations, such as general practitioners and specialists.
How to Fill Out the Patient Medical History Form Online (Step-by-Step)
Filling out the Patient Medical History Form online can be done easily using pdfFiller. Follow these steps:
-
Visit the pdfFiller platform and locate the Patient Medical History Form.
-
Gather necessary information, including current medications, allergies, and family medical history.
-
Fill in the required fields using the fillable form features.
-
Use checkboxes for yes/no options where applicable.
-
Sign the form digitally using the eSign feature.
-
Save your completed form for submission.
Review and Validation Checklist for the Patient Medical History Form
To ensure accuracy before submitting the Patient Medical History Form, consider the following checklist:
-
Verify that all required fields are signed, including those for guardians if applicable.
-
Check that all sections of the form are fully completed.
-
Avoid common pitfalls, such as leaving out vital health information.
-
Double-check the medical history provided for accuracy.
How to Sign the Patient Medical History Form
The signing process for the Patient Medical History Form includes various options:
-
Digital signatures that can be applied using pdfFiller.
-
Traditional wet signatures for those who prefer a physical signature option.
-
Guardians will need to sign on behalf of minor patients, fulfilling legal requirements.
Submitting the Patient Medical History Form
To submit your completed Patient Medical History Form, follow these guidelines:
-
Choose from submission methods: online, print, or email.
-
Be aware of deadlines associated with form submission.
-
Consider processing times when submitting the form to ensure timely review.
-
Confirm submission and track its status if possible.
Security and Compliance for the Patient Medical History Form
Handling sensitive medical information requires strict security measures. pdfFiller implements various security protocols:
-
256-bit encryption to protect user data.
-
HIPAA and GDPR compliance ensuring data privacy.
-
Guidance on securely retaining records after form completion.
Get Started with Your Patient Medical History Form Today!
Utilizing pdfFiller for your Patient Medical History Form needs offers numerous benefits. The platform features fillable forms, electronic signing, and efficient document management. Security measures are firmly in place to protect user data while providing a seamless experience.
How to fill out the patient medical history form
-
1.To begin, visit pdfFiller and search for the Patient Medical History Form or navigate directly if you have a link.
-
2.Upon opening the form, familiarize yourself with the layout, which includes various sections for your medical information.
-
3.Before filling out the form, gather necessary information, such as your current medications, allergies, and family medical history.
-
4.Ensure you have a reliable internet connection while working on the form, as it may auto-save your entries.
-
5.Start filling in the general medical information section, paying careful attention to accuracy in your responses.
-
6.Utilize the checkboxes for yes/no questions to indicate your medical history clearly and efficiently.
-
7.For signed portions of the form, use pdfFiller’s signature tools to add your signature digitally or print for manual signing.
-
8.Double-check all filled fields for any errors or omissions by reviewing the completed sections before saving.
-
9.Once you are satisfied with the completed form, click the save option to store your work on pdfFiller.
-
10.Decide how you want to submit the form: download it as a PDF, email it directly from pdfFiller, or print it for physical submission.

Who needs to fill out the Patient Medical History Form?
Patients, guardians of minor patients, and healthcare providers requiring detailed health information must fill out this form to ensure proper treatment.
What documentation is required when completing the form?
You should gather details such as current medications, previous health issues, allergies, and family medical history to accurately complete the form.
What happens if I make a mistake on the form?
If you make an error, review the entry and make corrections before saving or submitting. Ensure all information is accurate to avoid processing delays.
Can I submit the form electronically?
Yes, after completing the form on pdfFiller, you can submit it electronically by emailing it directly or downloading it for submission to your healthcare provider.
Is notarization required for this form?
No, the Patient Medical History Form does not require notarization, but signatures from the patient and guardian, if applicable, are necessary.
How long does it take to complete the form?
Completion time varies based on the individual's medical history but typically can take between 15 to 30 minutes.
What should I do if I need help completing the form?
If you need assistance, consult your healthcare provider or contact pdfFiller's support for guidance on using the platform.
Related Forms








If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.