Last updated on May 1, 2026
Get the free Kansas Decubitus Products Prior Authorization Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Kansas Decubitus Request
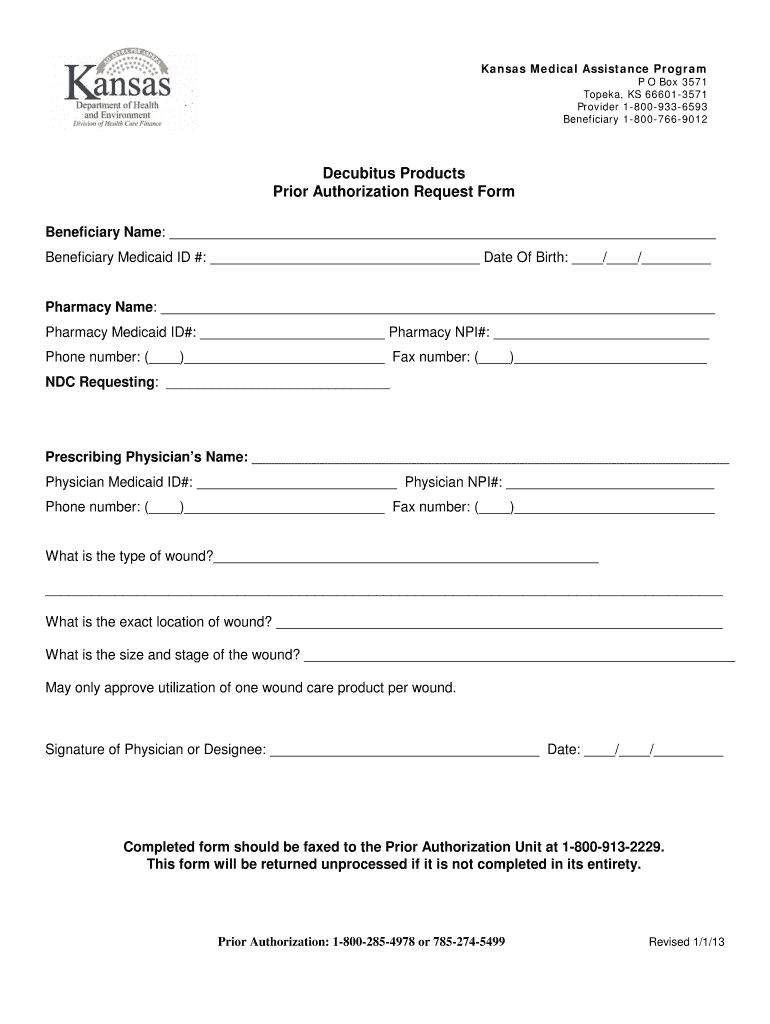
The Kansas Decubitus Products Prior Authorization Request Form is a healthcare document used by physicians to request prior authorization for wound care products for patients in Kansas.
pdfFiller scores top ratings on review platforms
Who needs Kansas Decubitus Request?
Explore how professionals across industries use pdfFiller.

Kansas Decubitus Request is needed by:
-
Healthcare providers in Kansas
-
Physicians prescribing decubitus products
-
Pharmacies processing medication requests
-
Clinics serving Medicaid patients
-
Medicaid beneficiaries requiring wound care products
Comprehensive Guide to Kansas Decubitus Request
What is the Kansas Decubitus Products Prior Authorization Request Form?
The Kansas Decubitus Products Prior Authorization Request Form is a vital document used by healthcare providers in Kansas to request prior authorization for decubitus (pressure ulcer) wound care products. This form ensures that patients receive timely access to necessary care through the Kansas Medical Assistance Program. It is specifically designed for healthcare practitioners such as physicians and specialists who interact with patients requiring these medical supplies.
Targeted primarily at healthcare providers, this form plays a critical role in facilitating requests and approvals, thereby connecting professionals with the resources they need to ensure effective treatment and support for their patients.
Purpose and Benefits of the Kansas Wound Care Authorization Request
The Kansas Wound Care Authorization Request form is essential for a variety of reasons. First and foremost, it facilitates timely access to necessary wound care products, which is crucial for patient recovery. By utilizing this form, healthcare providers can benefit in several ways.
-
Minimizes healing time for patients by ensuring they receive appropriate care promptly.
-
Ensures compliance with regulatory requirements and pre-authorization processes.
-
Supports claims for Medicaid or insurance coverage, helping patients manage costs effectively.
Key Features of the Kansas Decubitus Products Prior Authorization Request Form
This form includes several key features that streamline the authorization process. Essential fields capture detailed information, including:
-
Beneficiary information, critical for identifying the patient.
-
Physician details, which validate the request.
-
Pharmacy information for product fulfillment.
Additionally, the form has specific signature requirements and mandates supporting documents. Accurate information is crucial for a smooth approval process and prevents potential delays.
Who Needs the Kansas Decubitus Products Prior Authorization Request Form?
The Kansas Decubitus Products Prior Authorization Request Form is primarily for healthcare providers involved in patient care, particularly physicians and specialists who prescribe wound care products. Pharmacists and other stakeholders may also play a significant role in utilizing this form efficiently.
Patients often depend on this form when they require specific wound care products, which makes its proper completion vital for their treatment plans and overall recovery processes.
How to Fill Out the Kansas Decubitus Products Prior Authorization Request Form Online
Filling out the Kansas Decubitus Products Prior Authorization Request Form online via pdfFiller is straightforward. Follow these steps for accurate completion:
-
Access the form on pdfFiller without downloading it.
-
Enter required details such as Medicaid IDs and NPI numbers in the designated fields.
-
Verify all information for accuracy to ensure prompt processing.
Taking the time to confirm details before submission can significantly reduce errors and delays in patient care.
Submission Methods for the Kansas Decubitus Products Prior Authorization Request Form
After completing the Kansas Decubitus Products Prior Authorization Request Form, there are several submission methods available. The preferred method is to fax the completed document to the Prior Authorization Unit. Additionally, some electronic submission options may be available, providing flexibility in how the form is submitted.
It is important to adhere to submission deadlines to prevent any delays in patient care, ensuring that all necessary products are received in a timely manner.
Consequences of Not Filing or Late Filing the Kansas Decubitus Products Prior Authorization Request Form
Failing to file or submitting the Kansas Decubitus Products Prior Authorization Request Form late can lead to significant repercussions in patient care. Potential impacts include extended treatment timelines, which can adversely affect patient recovery and overall health.
Moreover, if the forms are incorrectly completed or submitted late, there is a heightened risk of claims denial. It is essential for healthcare providers to follow up diligently and advocate for their patients in such cases.
Security and Compliance for the Kansas Decubitus Products Prior Authorization Request Form
When filling out the Kansas Decubitus Products Prior Authorization Request Form, users can be assured of security and compliance. pdfFiller is committed to adhering to stringent security standards, including HIPAA and GDPR regulations.
Best practices for storing and transmitting sensitive health information are prioritized, with features such as encryption and secure access enhancing data protection. These measures provide peace of mind for healthcare providers handling sensitive patient information.
How to Leverage pdfFiller for Your Kansas Decubitus Products Prior Authorization Request Form
Utilizing pdfFiller for the Kansas Decubitus Products Prior Authorization Request Form offers numerous advantages. This platform allows for efficient filling, signing, converting, and sharing of PDFs entirely online, eliminating the need for downloads.
Moreover, the intuitive design of pdfFiller enhances efficiency in form completion and submission, making it easier for healthcare providers to manage these essential documents promptly and securely.
Example of a Completed Kansas Decubitus Products Prior Authorization Request Form
An example of a completed Kansas Decubitus Products Prior Authorization Request Form serves as a helpful guide for users. This visual representation or description helps elucidate the expected entries in each section, ensuring clarity during the completion process.
Commonly entered details will aid in understanding formatting guidelines, which are crucial for stakeholders to follow for accurate and actionable submissions.
How to fill out the Kansas Decubitus Request
-
1.Access the Kansas Decubitus Products Prior Authorization Request Form by visiting pdfFiller and using the search function to locate the form.
-
2.Once opened, familiarize yourself with the layout of the form. Use the toolbar to zoom in as needed for better clarity.
-
3.Gather all necessary patient information before starting, including beneficiary details, Medicaid IDs, and prescription specifics.
-
4.Begin filling in the beneficiary's name and contact details in the designated fields provided on the form.
-
5.Next, input the prescribing physician's information, ensuring to include their NPI number. Pay close attention to secure correct spelling.
-
6.For the pharmacy section, provide the complete details of the pharmacy, including contact information and any relevant pharmacy IDs.
-
7.Complete the sections that require specifics about the wound, including type, severity, and any pertinent medical notes or history.
-
8.Verify all entries for accuracy and ensure that all required fields are correctly filled out to prevent delays in processing.
-
9.After completing the form, locate the signature line and digitally sign or input your signature using pdfFiller’s tools.
-
10.When all information is reviewed, save the form on your device, ensuring to keep a copy for your records.
-
11.Finally, submit the completed form by faxing it to the Prior Authorization Unit as instructed, making sure to follow the submission guidelines provided by Medicaid.

What are the eligibility requirements for using this form?
The form is intended for use by healthcare providers in Kansas who prescribe decubitus products for Medicaid beneficiaries. Check with your local Medicaid office for specific eligibility criteria.
Are there deadlines for submitting this authorization request?
Typically, authorization requests should be submitted before the patient begins treatment or receives products. It is advisable to check with the Kansas Medical Assistance Program for specific timelines.
How can I submit the completed form?
Submit the completed Kansas Decubitus Products Prior Authorization Request Form by faxing it directly to the Prior Authorization Unit. Ensure that the fax number is current and listed on the form or official guidelines.
What supporting documents are needed with this form?
While the primary form details required beneficiary and physician information, additional documentation such as medical records or previous treatment notes may be necessary to support the request.
What are the common mistakes to avoid when filling out this form?
Common mistakes include incomplete information, incorrect beneficiary or physician details, and overlooking signatures. Double-check each section before submission to minimize errors.
What are the processing times for this prior authorization request?
Processing times may vary. However, requests are generally processed within a few business days. It’s advisable to follow up if you don’t receive confirmation within this timeframe.
What if I have concerns specific to this authorization request?
For form-specific concerns, consider reaching out directly to the Kansas Medical Assistance Program for clarification on any uncertainties regarding submission or processing.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.