Last updated on Mar 8, 2016
Get the free Atgam Coverage Determination Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
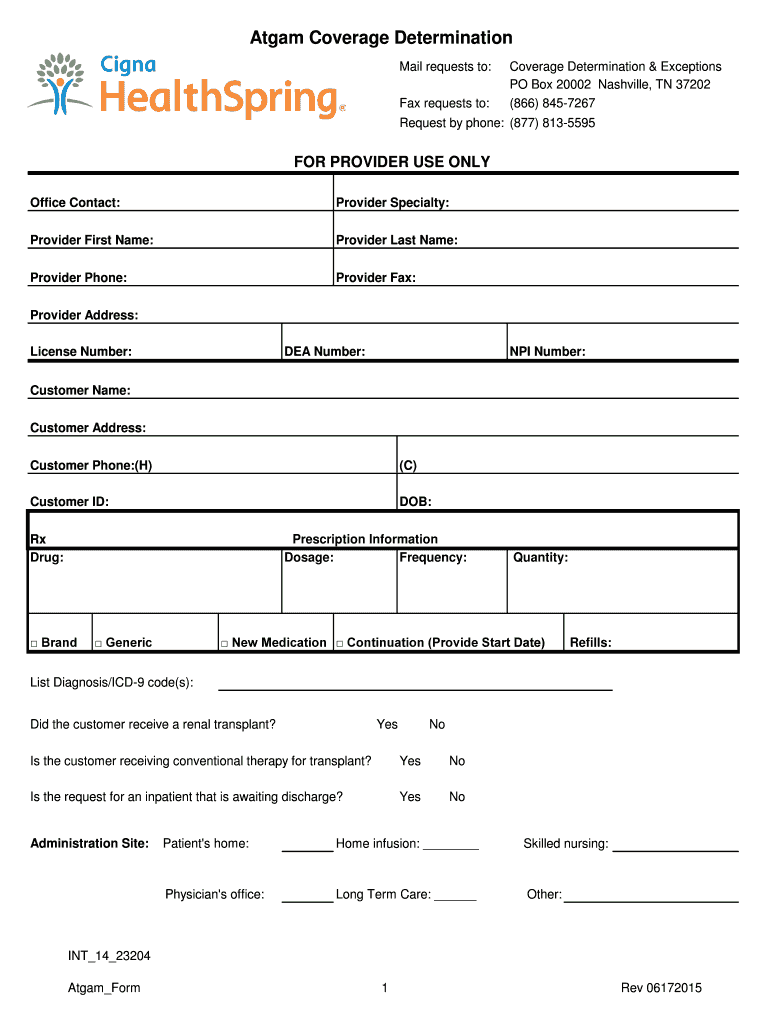
What is Atgam Coverage Form
The Atgam Coverage Determination Form is a medical consent document used by healthcare providers to request insurance coverage for the drug Atgam.
pdfFiller scores top ratings on review platforms
Who needs Atgam Coverage Form?
Explore how professionals across industries use pdfFiller.

Atgam Coverage Form is needed by:
-
Healthcare providers submitting coverage requests
-
Patients requiring Atgam for a medical procedure
-
Insurance representatives processing claims
-
Pharmacy staff prescribing Atgam
-
Medical practitioners specializing in renal transplants
-
Medical billing professionals managing claims
Comprehensive Guide to Atgam Coverage Form
What is the Atgam Coverage Determination Form?
The Atgam Coverage Determination Form is a critical document in healthcare, allowing providers to request coverage for the Atgam drug. This form plays a vital role in ensuring patients receive essential treatments for specific conditions, including renal diseases and certain autoimmune disorders. It is imperative for healthcare providers to utilize the Atgam coverage determination form to navigate the complexities of healthcare coverage requests effectively.
Purpose and Benefits of the Atgam Coverage Determination Form
Healthcare providers require the Atgam Coverage Determination Form to obtain timely approval for patient prescriptions. By leveraging this form, providers can expedite the coverage process and improve patient care outcomes. Key benefits include ensuring that the prescriptions are covered by insurance, which ultimately facilitates better treatment access for patients.
Key Features of the Atgam Coverage Determination Form
The Atgam Coverage Determination Form includes several important features designed for comprehensive completion. Sections within the form include:
-
Diagnosis codes relevant to the patient's condition
-
Detailed drug supply information
-
Provider certification requirements that affirm the need for the medication
Additionally, the form is designed to feature fillable fields for accurate and efficient data entry by healthcare providers.
Who Needs the Atgam Coverage Determination Form?
This form is primarily intended for healthcare providers who are responsible for submitting coverage requests to insurance companies. The completion of the Atgam Coverage Determination Form is necessary when initiating treatment plans that involve the Atgam drug, which may require specific documentation for approval.
How to Fill Out the Atgam Coverage Determination Form Online (Step-by-Step)
Filling out the Atgam Coverage Determination Form using pdfFiller involves a straightforward process. Follow these steps:
-
Access the Atgam Coverage Determination Form through pdfFiller.
-
Enter provider details, including name and contact information.
-
Input customer information such as name, address, and date of birth.
-
Detail the drug specifics, including dosage and frequency required.
-
Review all filled-out fields for accuracy before submission.
Each section of the form is clearly labeled to assist providers in accurately filling out the required information.
Review and Validation Checklist for the Atgam Coverage Determination Form
Accurate submission of the Atgam Coverage Determination Form is crucial to avoid delays. Providers should follow this validation checklist:
-
Verify that all fields are completed as required
-
Ensure all diagnosis codes accurately reflect the patient's condition
-
Check for any common errors, such as missing signatures or incomplete customer data
Paying attention to these details can significantly reduce the chances of rejection and subsequent resubmission.
Submission Methods and Delivery for the Atgam Coverage Determination Form
Healthcare providers have several options for submitting the completed Atgam Coverage Determination Form. Options include:
-
Online submission through the insurer's portal
-
Mailing the completed form to the designated insurance address
-
Faxing the form to ensure quick processing
It is essential to follow submission guidelines closely to ensure timely processing of coverage requests.
What Happens After You Submit the Atgam Coverage Determination Form
After submission of the Atgam Coverage Determination Form, providers can expect certain next steps. Processing timelines will vary based on several factors, including the insurer's workload and completeness of the submission. Providers should be aware of potential rejection reasons, which may include:
-
Inaccurate or incomplete information provided on the form
-
Lack of supporting documentation for the prescribed treatment
Healthcare providers should also know how to check the status of the application to stay informed about the approval process.
Security and Compliance for the Atgam Coverage Determination Form
Ensuring the security and compliance of all submitted information is paramount during the processing of the Atgam Coverage Determination Form. Sensitive patient information is protected through robust security measures, including:
-
256-bit encryption protocols for data transmission
-
Compliance with HIPAA and GDPR regulations to safeguard privacy
Providers can feel confident that their submissions are handled securely, protecting critical patient information throughout the process.
Streamline Your Atgam Coverage Determination Process with pdfFiller
pdfFiller is an ideal tool for healthcare providers looking to simplify the form-filling process for the Atgam Coverage Determination Form. Users can take advantage of its features to make the process seamless and efficient, ultimately aiding in better patient care delivery.
How to fill out the Atgam Coverage Form
-
1.Access pdfFiller and search for the Atgam Coverage Determination Form.
-
2.Click on the form to open it in the pdfFiller interface.
-
3.Gather necessary information such as provider and customer details, including names, contact information, and medical specifics.
-
4.Begin filling out the form by entering required fields like Provider First Name and Provider Last Name.
-
5.Continue by inputting the healthcare provider's phone number, fax number, and address.
-
6.Fill in the provider's medical credentials, including License Number, DEA Number, and NPI Number.
-
7.Next, enter the customer's information, such as Customer Name, Address, Phone, and Date of Birth.
-
8.Provide drug-related information, including the drug name (Atgam), dosage, frequency, and quantity needed.
-
9.Utilize checkboxes where applicable and ensure that all required fields are filled in accurately.
-
10.Make sure to carefully review the clinical information and expedite request options if necessary.
-
11.After completing all fields, thoroughly check the form for accuracy and completeness.
-
12.Once finalized, save your progress on pdfFiller, and select the option to download or submit the form electronically.
-
13.Follow any additional submission instructions provided by the insurance company, if necessary.

Who is eligible to use the Atgam Coverage Determination Form?
Eligibility to use the Atgam Coverage Determination Form typically involves healthcare providers submitting requests on behalf of patients needing Atgam for treatment. The patient must be covered under a Cigna plan for the request to be processed.
What information is required to complete the form?
To complete the Atgam Coverage Determination Form, you will need to provide detailed information about the healthcare provider, the patient, and the prescription. This includes diagnosis codes, renal transplant status, and other medical details.
How should I submit the completed Atgam form?
After completing the Atgam Coverage Determination Form on pdfFiller, you can submit your form electronically through the platform. Alternatively, print the form and submit it via mail or fax according to the insurance company's guidelines.
What are common mistakes to avoid when filling out this form?
Common mistakes include missing required fields, incorrect provider or patient details, and not reviewing for accuracy. Ensure that all medical information aligns with the patient's existing records.
What is the processing time for claims submitted using this form?
Processing times can vary based on the insurance provider's policies. Typically, you should expect a response within a few days to a couple of weeks, depending on whether expedited review was requested.
Are there any fees associated with using the Atgam Coverage Determination Form?
Generally, there are no direct fees for submitting the Atgam Coverage Determination Form itself. However, patients should check with their insurance provider regarding any associated costs or copays related to the drug Atgam.
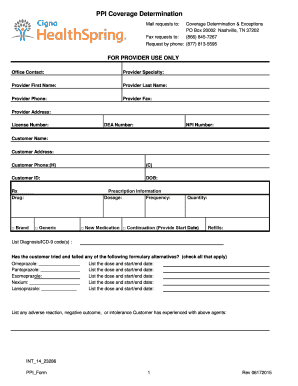
Related Forms






Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.