Last updated on Mar 8, 2016
Get the free Direct Reimbursement Claim Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Reimbursement Claim
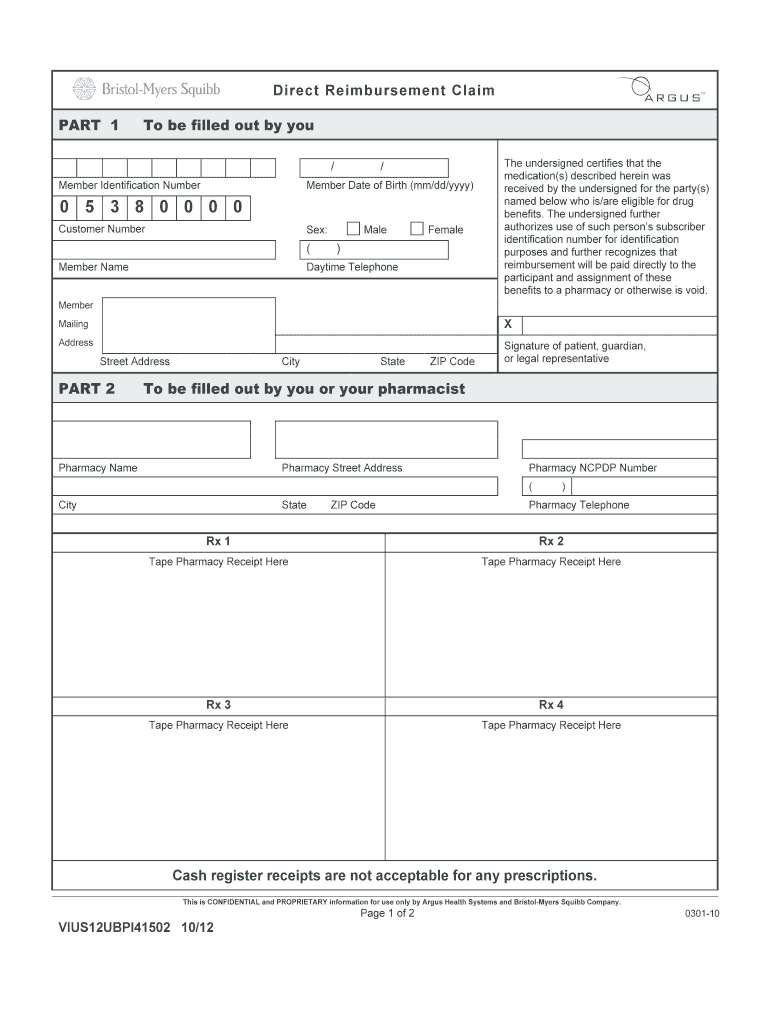
The Direct Reimbursement Claim Form is a medical billing document used by patients to request reimbursement for medication costs from Argus Health Systems and Bristol-Myers Squibb Company.
pdfFiller scores top ratings on review platforms
Who needs Reimbursement Claim?
Explore how professionals across industries use pdfFiller.

Reimbursement Claim is needed by:
-
Patients seeking reimbursement for medication expenses
-
Pharmacists assisting patients with reimbursement claims
-
Healthcare providers managing patient accounts
-
Insurance personnel verifying claims and reimbursements
-
Billing specialists handling medical billing inquiries
Comprehensive Guide to Reimbursement Claim
What is the Direct Reimbursement Claim Form?
The Direct Reimbursement Claim Form enables patients to submit claims for prescription reimbursements. This essential medical billing form is widely recognized in the healthcare industry, particularly when dealing with organizations like Argus Health Systems and Bristol-Myers Squibb. To complete the form correctly, users must provide specific member and pharmacy information, including member identification details and pharmacy receipts.
Purpose and Benefits of the Direct Reimbursement Claim Form
The primary purpose of the Direct Reimbursement Claim Form is to facilitate the reimbursement process for patients, making medical billing more efficient. Utilizing this healthcare claim form allows patients to quickly recover expenses for their prescription medications. It is crucial to file this form within 90 days of purchasing the prescription to avoid delays in reimbursement.
By adhering to these guidelines, patients can streamline the reimbursement process significantly.
Who Needs the Direct Reimbursement Claim Form?
This form is designed for patients seeking reimbursement for medications they have purchased out-of-pocket. Pharmacists play a vital role in helping patients understand when to use this pharmacy reimbursement form. Scenarios that may necessitate this form include instances where a patient pays for their medication upfront without insurance coverage.
Conversely, the claim form may not be needed in situations where medications are fully covered by insurance or government programs.
How to Fill Out the Direct Reimbursement Claim Form Online
Filling out the Direct Reimbursement Claim Form online is straightforward. Follow these steps:
-
Visit the designated online portal or platform.
-
Access the direct reimbursement claim form template.
-
Fill in required member details, including name, identification number, and date of birth.
-
Upload any necessary pharmacy receipts as proof of purchase.
-
Review the form for accuracy and completeness.
-
Submit the form electronically for processing.
Ensuring complete and accurate information in each field is critical to avoid processing delays.
Common Errors and How to Avoid Them
When completing the Direct Reimbursement Claim Form, mistakes can lead to claims being denied or delayed. Common errors include:
-
Missing required fields such as member name or pharmacy details.
-
Submitting incomplete receipts or documentation.
-
Errors in member identification numbers or dates of birth.
To avoid these pitfalls, implement a validation checklist and double-check all required fields before submission.
Submission Methods for the Direct Reimbursement Claim Form
Patients can submit their completed Direct Reimbursement Claim Form using several methods. Options include:
-
Postal mail to the designated processing address.
-
Digital submission through a secure online platform.
When submitting sensitive information, it's important to ensure secure methods are used. Be aware that there may be fees associated with the submission, and familiarize yourself with available payment methods for any applicable costs.
What Happens After You Submit Your Claim?
Once submitted, the claim undergoes processing. Patients can track the status of their submission, which may result in the following outcomes:
-
Claim approval with reimbursement issued.
-
Request for additional information to complete the claim.
-
Claim denial with provided reasons.
Understanding these outcomes helps patients navigate the reimbursement process effectively.
Security and Compliance for Your Submission
Data protection is paramount when submitting healthcare forms. pdfFiller employs robust security measures, including encryption and compliance with HIPAA and GDPR, ensuring the privacy of users filling out and submitting the Direct Reimbursement Claim Form.
How pdfFiller Can Simplify Your Direct Reimbursement Process
pdfFiller offers key features that significantly enhance the user experience when handling the Direct Reimbursement Claim Form. These benefits include:
-
eSigning capabilities for quicker processing.
-
Easy form management for all healthcare forms.
-
A streamlined interface for efficient document editing and submission.
Utilizing pdfFiller leads to a secure and efficient direct reimbursement process.
Sample Direct Reimbursement Claim Form
A visual example of a completed Direct Reimbursement Claim Form can guide users in accurately filling out their own claims. This sample outlines the key components needed to ensure no necessary information is overlooked. Users can also access downloadable templates within pdfFiller to assist them in their submissions.
How to fill out the Reimbursement Claim
-
1.Start by accessing pdfFiller and search for 'Direct Reimbursement Claim Form' using the search bar.
-
2.Open the form within the pdfFiller platform for editing.
-
3.Ensure to gather necessary information such as your Member Identification Number, Date of Birth, Member Name, and any pharmacy receipts before you begin filling.
-
4.Navigate to the required fields indicated on the form, clicking on each to enter your data.
-
5.Complete the Member Identification Number and fill in your personal details including your Date of Birth and Name in the designated fields.
-
6.In the pharmacy information section, provide the pharmacy's name and address from which you obtained the medications.
-
7.Be sure to upload or attach scanned copies of your pharmacy receipts using the upload option provided by pdfFiller.
-
8.Double-check all filled areas against the instructions provided on the form to ensure complete and accurate submission.
-
9.Once completed, review the entire form for any missing or incorrect information before proceeding.
-
10.Save your changes frequently to avoid losing any entered data as you work through the form.
-
11.To finalize the form, click on the submit option or download it in your preferred format.
-
12.After saving, you may choose to send the completed form by mail within the specified 90-day submission window.

Who is eligible to use the Direct Reimbursement Claim Form?
Eligible users include patients who purchased medications from participating pharmacies and need reimbursement from Argus Health Systems or Bristol-Myers Squibb for out-of-pocket expenses not covered by insurance.
What is the deadline for submitting the claim form?
The form must be completed and mailed within 90 days of the prescription purchase date to ensure eligibility for reimbursement.
How do I submit the Direct Reimbursement Claim Form?
The form should be mailed to the appropriate address as specified in the instructions once you have filled it out completely and attached all necessary documentation such as receipts.
What supporting documents are required with this form?
You must include pharmacy receipts showing the purchase of medications alongside the completed claim form. Ensure all information is accurate and legible.
What common mistakes should I avoid when filling out this form?
Ensure you complete all required fields and provide accurate information. Also, avoid leaving any sections blank, which could delay processing of your claim.
How long does it take to process the claim after submission?
Processing times may vary, but generally, you can expect a response within a few weeks after submission. Ensure that all documents are included to avoid delays.
Is this form required to be notarized?
No, the Direct Reimbursement Claim Form does not require notarization. However, all participant signatures must be provided where indicated.
Related Forms






Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.