Last updated on Mar 10, 2016
Get the free Oklahoma Workers' Compensation Physician Change Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
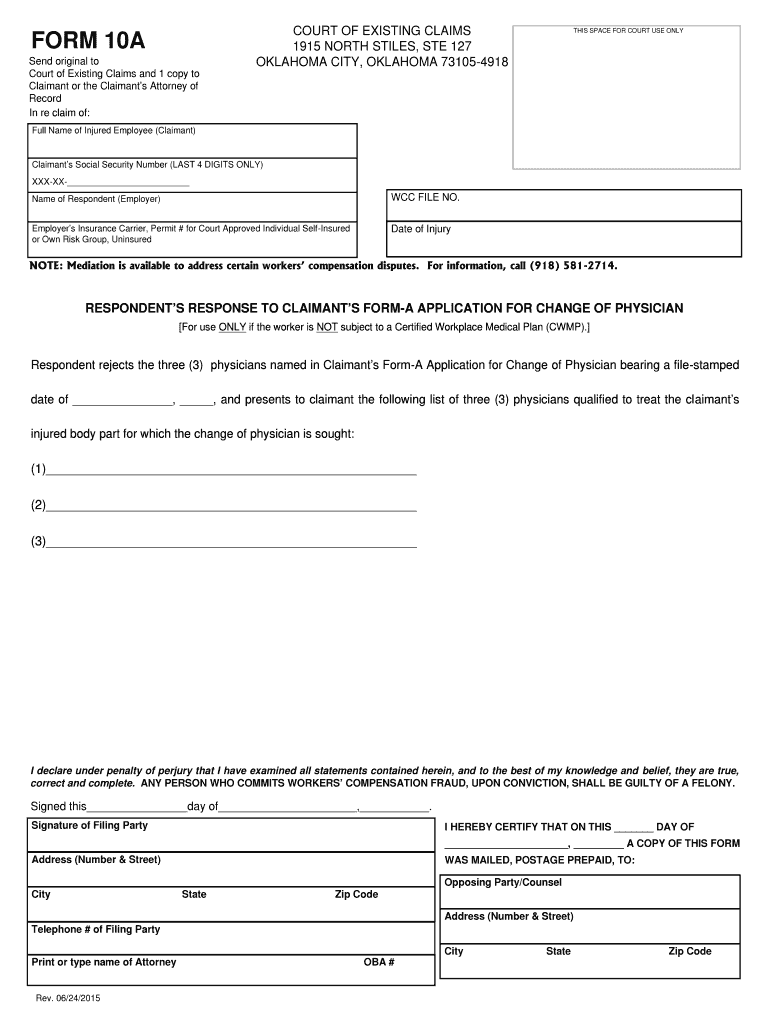
What is OK Physician Change Form
The Oklahoma Workers' Compensation Physician Change Form is a legal document used by respondents to formally reject a claimant's request to change their physician and propose three alternatives.
pdfFiller scores top ratings on review platforms
Who needs OK Physician Change Form?
Explore how professionals across industries use pdfFiller.

OK Physician Change Form is needed by:
-
Employers under Oklahoma workers' compensation laws
-
Insurance carriers handling claims in Oklahoma
-
Claimants seeking to change their physician
-
Legal professionals representing respondents
-
Staff assisting with workers' compensation claims
Comprehensive Guide to OK Physician Change Form
What is the Oklahoma Workers' Compensation Physician Change Form?
The Oklahoma Workers' Compensation Physician Change Form serves as an official document that allows respondents, typically employers or their insurance carriers, to formally reject a claimant's request to change physicians. This form is crucial for maintaining a clear record of the decision-making process regarding medical care for injured workers. It includes a stipulation that the respondent must sign under penalty of perjury, ensuring the authenticity of the submission.
Purpose and Benefits of the Oklahoma Workers' Compensation Physician Change Form
This form is vital for employers and insurance carriers since it helps in managing medical treatment decisions effectively and legally. By filling out the form correctly, respondents can ensure compliance with legal standards, which reduces the risk of disputes or litigation. Moreover, it facilitates transparent communication between all parties involved, promoting a smoother claims process.
Key Features of the Oklahoma Workers' Compensation Physician Change Form
The Oklahoma Workers' Compensation Physician Change Form consists of several important sections designed for user input. Key fields include the "Full Name of Injured Employee (Claimant)" and "Signature of Filing Party." Additional annotations throughout the form provide guidance, making it easier for users to complete the document accurately.
Who Needs the Oklahoma Workers' Compensation Physician Change Form?
The primary users of this form include employers, insurance carriers, and legal representatives in Oklahoma. These individuals or entities will need to utilize this document when an employee, who has filed a workers’ compensation claim, requests a change of physician. Understanding when to use this form is critical for both claimants and respondents as it impacts the direction of claims processing.
How to Fill Out the Oklahoma Workers' Compensation Physician Change Form Online (Step-by-Step)
-
Access the form through pdfFiller's platform.
-
Begin by entering the required information, including the injured employee’s full name.
-
Ensure all designated fields are filled correctly, paying attention to any optional sections.
-
Verify the accuracy of the information provided before proceeding.
-
After completion, ensure the form is signed by the filing party under penalty of perjury.
-
Follow any specific processing tips linked to the responsibilities of the submitting party.
Review and Validation Checklist for the Oklahoma Workers' Compensation Physician Change Form
Before submitting the form, it is important to conduct a thorough review to ensure completeness. Check for:
-
All required fields are filled accurately.
-
Proper signatures are included where necessary.
-
Common mistakes such as leaving required fields blank.
-
Consistency of information across all sections of the form.
Submission Methods for the Oklahoma Workers' Compensation Physician Change Form
Once the form is completed, it must be submitted correctly to be effective. Options for submission include mailing the completed form to the opposing party involved in the claim. Be mindful of any applicable deadlines to ensure that all parties are informed timely about the physician change.
Security and Compliance When Handling the Oklahoma Workers' Compensation Physician Change Form
pdfFiller implements robust security measures to protect sensitive information during the processing of documents such as the Oklahoma Workers' Compensation Physician Change Form. Compliance with both HIPAA and GDPR standards ensures that users' privacy is maintained throughout the handling of personal data.
Why Use pdfFiller for the Oklahoma Workers' Compensation Physician Change Form?
Using pdfFiller for the Oklahoma Workers' Compensation Physician Change Form offers numerous advantages. The platform provides user-friendly features that simplify the creation, filling, and electronic signing of the form. Its capabilities for document management enhance efficiency, making the entire process safer and more organized.
Next Steps After Submitting the Oklahoma Workers' Compensation Physician Change Form
After submitting the form, users should track the status of their submission to confirm its receipt by the opposing party. In the event that the submission is rejected or requires amendments, users should be prepared to take appropriate actions. It is also advisable to maintain copies of the completed form for personal records and reference.
How to fill out the OK Physician Change Form
-
1.To begin, access the Oklahoma Workers' Compensation Physician Change Form on pdfFiller. Use the search bar or navigate through the legal forms section to locate it easily.
-
2.Once you open the form, familiarize yourself with the layout, which includes sections for the 'Full Name of Injured Employee (Claimant)', 'Signature of Filing Party', and additional fields for alternative physicians.
-
3.Before filling out the form, gather all necessary information, including the claimant's details and the names and contact information of three alternative physicians you wish to propose.
-
4.Use pdfFiller’s interactive features to fill in the required fields. Click on the blank spaces to type in your information directly using your keyboard or select options available in dropdown menus.
-
5.If there are checkboxes, click on them to make your selections clear. Ensure you follow the instructions to provide complete information regarding each field.
-
6.After completing the form, review all entries to check for accuracy and completeness. Use the review function on pdfFiller to verify that all required fields are filled out correctly.
-
7.Once everything is accurate, finalize the form. pdfFiller allows you to save or download your completed form in PDF format or submit it directly through the platform if applicable.
-
8.Make sure to email or mail a signed copy of the form to the opposing party as required under penalty of perjury. Retain a copy for your records.

Who is eligible to fill out the Oklahoma Workers' Compensation Physician Change Form?
Eligibility to fill out this form generally includes employers or their insurance carriers responding to a claimant's request for a physician change in Oklahoma workers' compensation cases.
What happens if I miss the submission deadline?
Missing the submission deadline may result in complications regarding the request for a physician change. It is essential to submit the form timely to avoid any adverse consequences related to the case.
How can I submit the Oklahoma Workers' Compensation Physician Change Form?
You can submit the completed form by mailing a signed copy to the opposing party. Additionally, if allowed, you may submit it electronically through platforms like pdfFiller.
What supporting documents do I need to provide with the form?
Typically, you should include any relevant documentation related to the claimant's current physician and the proposed alternative physicians. Ensure all relevant information is included to support your decision.
What are common mistakes to avoid when filling out the form?
Common mistakes include leaving mandatory fields blank, incorrect or illegible entries, and failing to sign under penalty of perjury. Always double-check your work before submission.
How long does it take to process the form?
Processing times can vary, but it generally depends on the responding party's review and any legal timelines in your jurisdiction. Checking with your legal representative can provide more specific estimates.
Can I modify the form after submission?
Once submitted and depending on state regulations, modifications may be challenging. It is best to ensure the form is accurate before submitting to prevent the need for changes later.
Related Forms







Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.