Last updated on Mar 10, 2016

Get the free Authorization to Disclose Protected Health Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is PHI Disclosure Authorization
The Authorization to Disclose Protected Health Information is a healthcare form used by patients to grant permission for the disclosure of their medical records.
pdfFiller scores top ratings on review platforms
Who needs PHI Disclosure Authorization?
Explore how professionals across industries use pdfFiller.

PHI Disclosure Authorization is needed by:
-
Patients seeking to authorize medical record sharing
-
Healthcare providers needing consent for information release
-
Insurance companies requiring medical history verification
-
Legal representatives managing health information
-
Family members assisting patients in medical matters
Comprehensive Guide to PHI Disclosure Authorization
What is the Authorization to Disclose Protected Health Information?
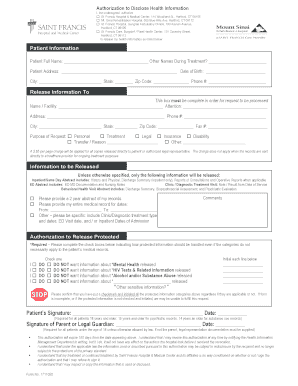
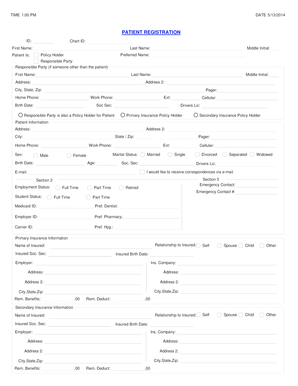
The Authorization to Disclose Protected Health Information (PHI) is a vital form in healthcare that allows patients to consent to the release of their medical records. This form ensures that patient information is shared only with authorized entities, safeguarding privacy rights while facilitating necessary information exchange. Essential components of this form include patient information, recipient details, and specifics regarding the information to be disclosed.
Key components essential for the authorization process cover patient identifiers like name, date of birth, and contact details, ensuring clarity in the disclosure. Patients may find terms like “authorization to disclose protected health information” and “medical records release” pertinent when discussing their options for sharing sensitive data.
Purpose and Benefits of the Authorization to Disclose Protected Health Information
This authorization form serves a crucial purpose in enforcing patient rights over their health information, providing explicit consent for its disclosure. By implementing this form, patients can enjoy seamless communication with their healthcare providers, enhancing the overall efficiency of medical care. The importance of understanding one’s rights surrounding health information cannot be overstated.
Using a patient consent form significantly streamlines the process of obtaining and sharing medical records. This authorization empowers patients to manage who accesses their data, creating a sense of control and security in a highly sensitive area of personal information.
Key Features of the Authorization to Disclose Protected Health Information
The Authorization to Disclose Protected Health Information includes several essential features designed for clarity and ease of use. The form comprises fillable fields for entering pertinent patient information, such as the patient's name, date of birth, and contact information. Additionally, the form incorporates checkboxes that specify types of information covered and the purposes for which it is being disclosed.
This structured format promotes better understanding and compliance while ensuring that the requirements for phi disclosure authorization are met efficiently. For instance, patients will find sections that help identify the medical form being used and the particular information being authorized for release.
Who Needs the Authorization to Disclose Protected Health Information?
This authorization form may be required in a variety of scenarios, especially when transferring care or obtaining treatment records. Specific individuals or entities—including healthcare providers, family members, or institutions—could demand this authorization to ensure the lawful sharing of sensitive health data.
Moreover, understanding who needs the authorization is critical for maintaining proper health information management. Scenarios necessitating the use of this form can extend widely across different healthcare contexts, each highlighting the importance of patient consent in protecting personal health information.
How to Fill Out the Authorization to Disclose Protected Health Information Online
Completing the Authorization to Disclose Protected Health Information online through pdfFiller is straightforward. Begin by entering the required patient information into the designated fields, ensuring accuracy in details like the patient’s name and date of birth. Next, select the appropriate checkboxes to indicate which types of information are authorized for release.
Completing the form accurately is essential for a smooth submission process. Check each filled field before submission to avoid common errors, ensuring that every necessary detail is provided and all checkboxes are relevant and selected.
Submission Methods for the Authorization to Disclose Protected Health Information
Once the Authorization to Disclose Protected Health Information is completed, users can choose from several submission methods to send their form. Online submission through pdfFiller offers convenience and speed, allowing for efficient processing.
Additionally, users may opt to mail or deliver the completed form in person, depending on their preference and the specific requirements of the receiving entity. Each submission method offers a different experience, ensuring flexibility for users based on their needs.
Security and Compliance Considerations for the Authorization to Disclose Protected Health Information
The protection of sensitive health information is paramount, and pdfFiller takes this responsibility seriously. With security measures such as encryption, the platform ensures compliance with HIPAA and GDPR regulations, safeguarding personal health data from unauthorized access.
Understanding the importance of these security measures helps health information authorization users feel reassured about the safety of their data. Particularly in healthcare, maintaining high standards of confidentiality is not only a legal requirement but also an essential aspect of patient care.
What to Expect After Submitting the Authorization to Disclose Protected Health Information
After submitting the Authorization to Disclose Protected Health Information, patients typically receive information regarding the processing timeline. Knowing how long the submission will take can help set expectations and ease concerns about delays.
Patients should also be aware of possible next steps following submission, including how to check the status of their authorization and when it becomes effective. This proactive approach enhances the user experience and enables smoother interactions between patients and healthcare entities.
Why Choose pdfFiller for Your Authorization to Disclose Protected Health Information?
Choosing pdfFiller for completing and submitting the Authorization to Disclose Protected Health Information streamlines the process. The platform’s user-friendly interface and cloud-based services simplify filling and eSigning forms, ensuring a quick and efficient experience.
Moreover, pdfFiller emphasizes security features and adherence to legal compliance, reassuring users that their sensitive information is handled with care. Utilizing a reliable platform helps maintain the critical nature of health information during disclosure processes.
Sample Authorization to Disclose Protected Health Information
Providing users with a sample Authorization to Disclose Protected Health Information can serve as a helpful reference. This visual guide illustrates how the completed form should look, clarifying uncertainties and common mistakes encountered when filling out the document.
A well-structured example highlights crucial points of focus, ensuring that patients feel confident in complying with the requirements of this form. Understanding the right approach in completing this type of authorization is invaluable for effective healthcare communication.
How to fill out the PHI Disclosure Authorization
-
1.To access the Authorization to Disclose Protected Health Information form on pdfFiller, visit the website and use the search bar to enter the form's name.
-
2.Once located, click on the form to open it in the pdfFiller interface, which allows for easy navigation and editing.
-
3.Before you start filling out the form, gather essential information such as your name, date of birth, address, contact information, and details of the entity to which you want to disclose records.
-
4.Begin filling in the fields by clicking on each blank area. Type in your personal information directly into the form fields provided in the pdfFiller editor.
-
5.If you need to specify the type of information being disclosed, use the checkboxes provided in the form to mark your choices clearly.
-
6.Ensure that you fill out the purpose of disclosure section, which helps to clarify why the information is being shared.
-
7.After completing the form, review all information for accuracy and completeness. This can be done by using the preview feature in pdfFiller.
-
8.Once you are satisfied with the form, proceed to save the document. You can download it to your device or opt to submit it electronically if required by the receiving entity.
-
9.If you choose to submit electronically, follow the instructions for email submission within pdfFiller, which may include uploading the form directly to the recipient's portal or sending it via email.

Who is eligible to complete this form?
Patients or their authorized representatives are eligible to complete the Authorization to Disclose Protected Health Information form for medical record sharing.
What information do I need to complete this form?
You need your personal information, including your name, date of birth, address, and the details of the entity receiving your medical records.
How long is the authorization valid?
This form's authorization is valid for one year unless otherwise specified, meaning it will expire after this period unless renewed by the patient.
How do I submit this form once completed?
You can submit the completed form electronically via pdfFiller or download it and send it directly to the designated entity by mail or email.
Are there common mistakes to avoid when filling in this form?
Common mistakes include omitting required fields, incorrect checkboxes for information type, and forgetting to sign and date the form before submission.
Can I revoke this authorization after signing?
Yes, you can revoke this authorization at any time in writing, but be aware that it cannot affect any disclosures made prior to the revocation.
Is notarization required for this form?
No, this Authorization to Disclose Protected Health Information does not require notarization, simplifying the process for patients.
Related Forms





Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.