Last updated on Mar 10, 2016
Get the free Authorization to Release Medical Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
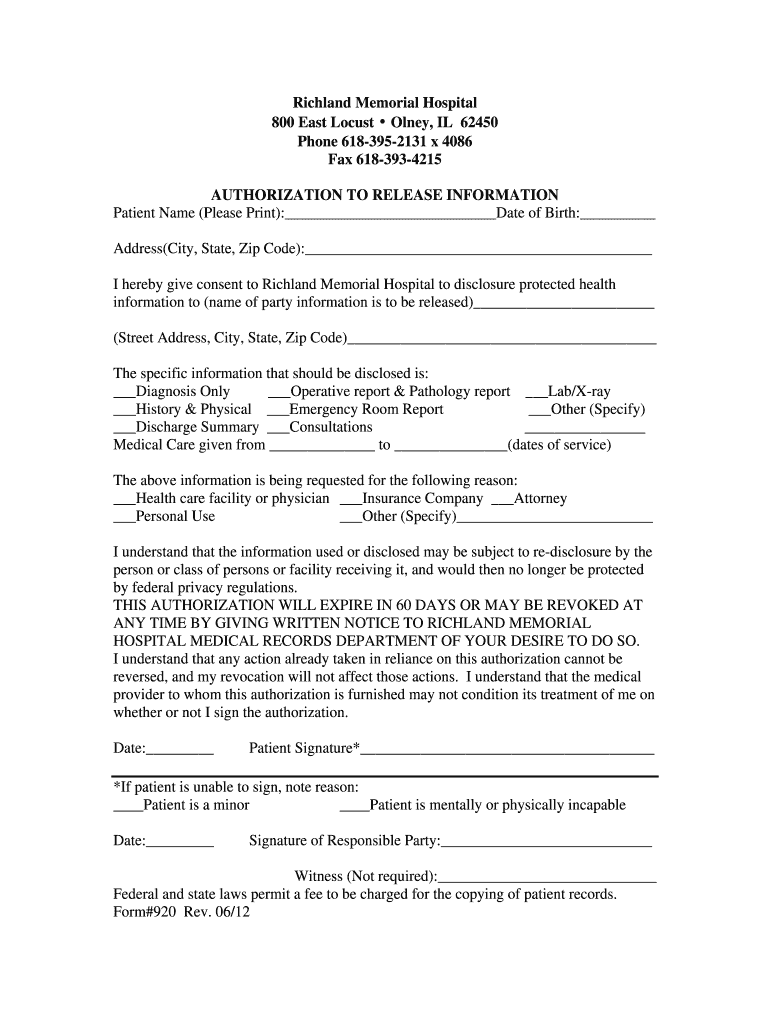
What is Medical Release Form
The Authorization to Release Medical Information is a healthcare form used by patients to consent to the disclosure of their protected health information to specified parties.
pdfFiller scores top ratings on review platforms
Who needs Medical Release Form?
Explore how professionals across industries use pdfFiller.

Medical Release Form is needed by:
-
Patients of Richland Memorial Hospital
-
Responsible parties managing patient care
-
Healthcare providers requesting medical records
-
Insurance companies needing patient information
-
Legal representatives needing health disclosures
-
Researchers or clinical study coordinators
Comprehensive Guide to Medical Release Form
What is the Authorization to Release Medical Information?
The Authorization to Release Medical Information form is a crucial document within the healthcare process, allowing patients to provide consent for disclosing their protected health information. This medical release form acts as a formal request for healthcare providers to share patient data with other entities.
Obtaining patient consent is essential for compliance with privacy regulations, ensuring that individuals maintain control over who accesses their medical information. This authorization is especially significant when dealing with sensitive health data and supports transparency in healthcare practices.
Purpose and Benefits of the Authorization to Release Medical Information
This authorization form serves a multifaceted purpose in the healthcare ecosystem, benefiting both patients and providers. It simplifies the process of sharing medical records while complying with HIPAA regulations, ensuring that patient health information is handled securely and within legal bounds.
Patients gain control over their medical history, streamlining interactions with healthcare providers and facilitating collaboration among various professionals involved in their care. The health information release enhances the quality of care through effective communication and information sharing.
Key Features of the Authorization to Release Medical Information
The Authorization to Release Medical Information form includes several key elements that ensure comprehensive data collection. Required fields such as patient name, date of birth, and address help identify the individual within healthcare systems.
Additionally, the form features checkboxes that allow patients to specify which information they wish to disclose, such as diagnosis and lab results. This healthcare privacy form is designed to be straightforward, promoting clarity in what information is shared.
Who Needs the Authorization to Release Medical Information?
The primary target users of the Authorization to Release Medical Information form are patients and their responsible parties. Situations that necessitate using this form include seeking second opinions, transferring records to new healthcare providers, or granting access to caregivers.
By obtaining a patient signature form, healthcare providers can ensure they are complying with privacy laws while respecting patient autonomy in managing their health information.
How to Fill Out the Authorization to Release Medical Information Online (Step-by-Step)
Completing the Authorization to Release Medical Information form online can be done efficiently by following these step-by-step instructions:
-
Start by entering your patient name and date of birth clearly.
-
Provide your current address for identification purposes.
-
Select the specific information to be released by checking the appropriate boxes.
-
Identify the recipient who will receive this information, including their name and contact details.
-
Specify the reason for the request in the designated field.
-
Provide your signature or that of a responsible party if applicable.
Digital Signature vs. Wet Signature Requirements
This section clarifies the signing requirements associated with the Authorization to Release Medical Information. A digital signature is permissible if it adheres to legal standards, allowing for efficient processing and quicker turnaround times.
For instances where a responsible party's signature is necessary, it is essential to indicate their relationship to the patient, ensuring that authorization is valid under HIPAA regulations.
Submission Methods and Delivery of the Authorization to Release Medical Information
Once the form is completed, various submission methods are available for sending the Authorization to Release Medical Information. Options include electronic submission through secured channels, physical mailing, or delivering the form in person to the appropriate healthcare office.
Tracking submissions and ensuring receipt confirmation are crucial steps in maintaining a record of the authorization process, ultimately safeguarding patient information throughout his journey.
What Happens After You Submit the Authorization to Release Medical Information?
After submitting the Authorization to Release Medical Information, you can expect certain protocols to unfold. The processing timelines may vary, but healthcare facilities typically acknowledge receipt and begin the review process promptly.
Patients can also follow up to check the application status, ensuring that their requests are being handled efficiently and accurately.
Common Errors and How to Avoid Them When Filling Out the Authorization to Release Medical Information
Filling out the Authorization to Release Medical Information form requires attention to detail to avoid common errors. Mistakes such as omitting vital information or failing to sign can delay the processing of records.
To minimize errors, consider these tips: double-check all fields, ensure clarity in your handwriting, and confirm that the signatures are complete and legible before submission. Taking these steps promotes accuracy and expedites the release process.
Experience Seamless Form Completion with pdfFiller
PdfFiller offers users an exceptional platform for filling out the Authorization to Release Medical Information form. With its robust capabilities, users can create securely edited documents quickly and easily.
Utilizing pdfFiller ensures the form is completed with high standards of security, allowing for a more straightforward and efficient process in managing sensitive medical information seamlessly.
How to fill out the Medical Release Form
-
1.Access the Authorization to Release Medical Information form on pdfFiller by searching for it in the template library or using the direct link provided by your healthcare provider.
-
2.Open the form in pdfFiller's editor. Familiarize yourself with the layout, including fillable fields and checkboxes.
-
3.Gather the required information before starting. This includes the patient's name, date of birth, complete address, and any specific medical information to be released.
-
4.Begin by filling out the patient's personal details in the designated fields. Ensure all information is correct and up-to-date.
-
5.Use checkboxes to indicate which specific health information you wish to disclose, such as diagnosis, lab results, or operative reports.
-
6.Specify the purpose for which the information is being released, providing detailed reasoning where needed.
-
7.Include the date and signature of the patient in the appropriate sections. If the patient is unable to sign, a responsible party must also provide their signature.
-
8.Review all entries for accuracy. Verify that the provided information is complete and that the form reflects the patient's intentions.
-
9.Finalize the form by saving your changes. Use the 'Save' function to ensure all filled information is stored securely.
-
10.Download a copy of the completed form for your records or submit it directly through pdfFiller if required by Richland Memorial Hospital.

Who is eligible to fill out the Authorization to Release Medical Information form?
Any patient of Richland Memorial Hospital can fill out this form to authorize the release of their medical information. Additionally, a responsible party may complete the form on behalf of a patient unable to sign.
What is the validity period of this authorization?
The Authorization to Release Medical Information remains valid for 60 days from the date of signature. After this period, a new authorization will need to be completed.
How should I submit the completed form?
You can submit the completed Authorization to Release Medical Information form directly to Richland Memorial Hospital's medical records department. If required, you may also be able to submit it through pdfFiller's submission options.
What supporting documents do I need when submitting this form?
Typically, no additional supporting documents are required when submitting this authorization form. However, if the patient is unable to sign, proof of relationship or authority may be needed.
What common mistakes should I avoid while filling out this form?
Ensure all information is complete and accurate, particularly patient identification details and specific information to be disclosed. Missing signatures or details can lead to delays in processing.
How long will it take to process the authorization request?
Processing times can vary but typically, you should allow a few days for the hospital to process the authorization once submitted. It's best to verify with the hospital for specific timeframes.
Can I revoke my authorization after submitting this form?
Yes, you can revoke your authorization to release medical information at any time. To do this, a written notice must be submitted to Richland Memorial Hospital's medical records department.
Related Forms




Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.