Last updated on Mar 10, 2016

Get the free Request to Restrict Disclosure of Medical Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
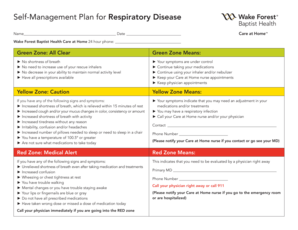
What is Medical Disclosure Restriction
The Request to Restrict Disclosure of Medical Information is a healthcare form used by patients or their representatives to request that a healthcare provider not disclose specific medical information to their health plan.
pdfFiller scores top ratings on review platforms
Who needs Medical Disclosure Restriction?
Explore how professionals across industries use pdfFiller.

Medical Disclosure Restriction is needed by:
-
Patients seeking to restrict medical information disclosure
-
Personal representatives of patients managing healthcare privacy
-
Healthcare providers needing to understand patient privacy requests
-
Legal guardians or advocates for patients
-
Health plan administrators requiring updated permission forms
Comprehensive Guide to Medical Disclosure Restriction
What is the Request to Restrict Disclosure of Medical Information?
The Request to Restrict Disclosure of Medical Information serves a vital role in protecting patient privacy. This form enables patients or their representatives to request specific restrictions on what medical information can be disclosed to health plans. Ensuring the confidentiality of medical records not only upholds patient rights but also fosters a trusting relationship between patients and healthcare providers. By utilizing this patient privacy form, individuals can assert control over their sensitive data.
Why Use the Request to Restrict Disclosure of Medical Information?
This medical disclosure restriction form offers significant advantages for both patients and their representatives. By using it, individuals can effectively control the sharing of their medical information with health plans, ensuring privacy and enhancing confidentiality. This process empowers patients, reinforcing their rights and enabling better management of their healthcare information. Adopting this approach helps maintain trust and aligns with contemporary privacy standards.
Who Needs the Request to Restrict Disclosure of Medical Information?
Patients and their personal representatives are the primary users of the Request to Restrict Disclosure of Medical Information. It is crucial for these individuals to understand when this form is necessary. Common scenarios prompting the use of this form include:
-
When a patient wishes to limit access to specific medical records.
-
If the patient has concerns about their health plan's disclosure practices.
-
When a personal representative needs to advocate for a patient’s privacy requests.
Key Components of the Request to Restrict Disclosure of Medical Information Form
The request form comprises several important components that users must complete accurately. Key sections include the name of the health plan, details about the services or items subject to restriction, and contact information for the patient. Additionally, the form requires signatures from both patients and their representatives, along with an agreement to cover the costs of services. This structure ensures clarity in communication and compliance with privacy preferences.
How to Fill Out the Request to Restrict Disclosure of Medical Information Form Online
Completing the Request to Restrict Disclosure of Medical Information form through pdfFiller is a straightforward process. To fill it out effectively, follow these steps:
-
Access the pdfFiller platform and locate the form.
-
Fill in the blank fields with your personal and medical information.
-
Use checkboxes to indicate the specific disclosures to restrict.
-
Provide your signature electronically to finalize the submission.
This user-friendly platform enhances accessibility, making it easier for patients to manage their privacy preferences.
Filing and Submitting the Request to Restrict Disclosure of Medical Information
After completing the form, it is essential to know how to submit it properly. The request must be sent to the appropriate health plan or directly to the UH Privacy Officer. Submission methods can include:
-
Emailing the completed form.
-
Mailing a physical copy to the designated contact.
Following up on the submission is also critical, ensuring that the request has been received and processed in a timely manner.
Consequences of Not Filing the Request to Restrict Disclosure
Failing to submit the Request to Restrict Disclosure of Medical Information may lead to significant risks regarding medical privacy. Such consequences can include unauthorized disclosures of sensitive health information and potential breaches of patient rights. It is vital for patients to act promptly and file the request to safeguard their medical data effectively.
Security and Compliance with the Request to Restrict Disclosure of Medical Information
When dealing with sensitive medical information, security is paramount. pdfFiller employs robust security measures, ensuring compliance with HIPAA and GDPR regulations. Users can feel confident in the knowledge that their medical information is secure and protected while utilizing this platform. This commitment to data protection underscores the importance of patient privacy during the form-filling process.
How pdfFiller Helps You with the Request to Restrict Disclosure of Medical Information
pdfFiller offers a range of features tailored to assist users in managing the Request to Restrict Disclosure of Medical Information effectively. Key benefits include:
-
eSigning options for convenient electronic signatures.
-
Form customization capabilities to meet individual needs.
-
Safe storage for easy access to completed forms.
Patients can leverage these tools to ensure that their submissions are accurate and securely handled.
Get Started with the Request to Restrict Disclosure of Medical Information Today!
Now is the time to take control of your medical information. Utilizing pdfFiller simplifies the process of filling out the Request to Restrict Disclosure of Medical Information. By accessing the platform, you can efficiently complete your request and enhance your privacy management. Taking this step empowers you to protect your sensitive information with ease.
How to fill out the Medical Disclosure Restriction
-
1.Begin by accessing the pdfFiller website and log in to your account or create a new account if you don't have one.
-
2.Once logged in, use the search bar to locate the 'Request to Restrict Disclosure of Medical Information' form.
-
3.Click on the form to open it in the pdfFiller interface.
-
4.Before filling out the form, gather necessary information including your healthcare services details, health plan name, and your contact information.
-
5.Navigate the fields in the form, beginning with your full name where it indicates. Use pdfFiller's type tool for easy text input.
-
6.Continue completing sections that require health service descriptions and health plan details by clicking on each blank field.
-
7.If there are any checkboxes, click to mark them according to your agreement to the outlined restrictions.
-
8.Review the completed form carefully, ensuring all fields are filled correctly and legibly.
-
9.Finalize your form by generating a digital signature if required; pdfFiller offers tools to create and insert your signature.
-
10.Once you're satisfied with the form's content, choose the save option to keep a copy within your pdfFiller account.
-
11.To submit the form, use the email option to send directly to the UH Privacy Officer or download the PDF for printing and mailing.

Who is eligible to use this form?
The form is designed for patients or their authorized representatives who wish to restrict the disclosure of specific medical information to their health plans, ensuring privacy in healthcare matters.
Are there any deadlines for submitting this form?
While there are no universally mandated deadlines, it is advisable to submit the form as soon as your decision to restrict disclosure is made to prevent any unauthorized sharing of information.
How do I submit the completed form?
You can submit the completed form by emailing it directly to the UH Privacy Officer or printing it and sending it via postal mail. Make sure to check the submission preferences or requirements beforehand.
What supporting documents are required with this form?
Typically, no additional documents are required when submitting this form. However, it can be helpful to include any relevant identification or authorization letters from personal representatives.
What common mistakes should I avoid when filling out this form?
Common mistakes include leaving mandatory fields blank, failing to provide a complete description of the medical information to be restricted, or not signing the form. Double-check for errors before submission.
How long does it take to process this restriction request?
Processing times can vary depending on the healthcare provider’s procedures, but typically, requests should be acknowledged within a few business days and processed promptly.
Can I withdraw my request after submitting this form?
Yes, you can withdraw your request at any time. It is advisable to notify the healthcare provider in writing to ensure the request is formally canceled.
Related Forms








Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.