Last updated on Mar 13, 2016

Get the free Antirheumatic Agents Prior Authorization Review Request
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
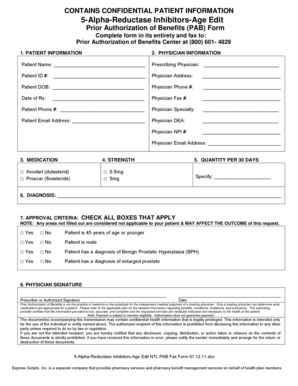
What is Prior Authorization Request
The Antirheumatic Agents Prior Authorization Review Request is a healthcare form used by physicians to request prior authorization for antirheumatic medications.
pdfFiller scores top ratings on review platforms
Who needs Prior Authorization Request?
Explore how professionals across industries use pdfFiller.

Prior Authorization Request is needed by:
-
Healthcare providers seeking medication approval
-
Physicians treating patients with rheumatoid arthritis
-
Pharmacy management departments processing requests
-
Insurance companies evaluating prior authorization requests
-
Patients requiring treatment with specific antirheumatic agents
Comprehensive Guide to Prior Authorization Request
Overview of the Antirheumatic Agents Prior Authorization Review Request
The Antirheumatic Agents Prior Authorization Review Request is crucial in the healthcare system, serving as a formal communication tool to secure approval for antirheumatic medications. This form facilitates vital access to treatment for patients diagnosed with rheumatoid arthritis. Key stakeholders, including healthcare providers and Pharmacy Management, play significant roles in the completion and submission of this prior authorization request form, enhancing the efficiency of medication approval processes.
Purpose and Benefits of the Antirheumatic Agents Prior Authorization Review Request
This form is critical for ensuring that patients gain access to necessary treatments. By effectively using this medication approval form, healthcare providers can secure timely authorization for antirheumatic medications, which can significantly improve patient outcomes. Moreover, the timely completion of prior authorization requests leads to enhanced treatment access for patients and a streamlined process for healthcare providers.
Who Needs the Antirheumatic Agents Prior Authorization Review Request?
The primary users of the Antirheumatic Agents Prior Authorization Review Request are healthcare providers who submit this documentation to obtain necessary treatment approvals. Physicians play an essential role by signing the form to confirm the patient's medical necessity. Specifically, prior authorization is often required for patients who have not responded adequately to previous medication therapies, thereby ensuring they receive appropriate care.
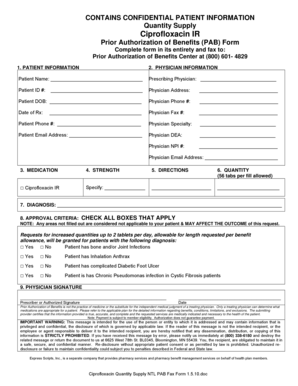
How to Fill Out the Antirheumatic Agents Prior Authorization Review Request Online (Step-by-Step)
Completing the prior authorization request form requires careful attention to detail. Begin by reviewing the form structure to understand key sections that must be filled out. Follow these steps for successful completion:
-
Provide patient details, including full name and date of birth.
-
Enter the diagnosis, ensuring accuracy regarding the patient's condition.
-
Include information on previous medications the patient has tried.
-
Offer a clear medical justification outlining the need for the requested medication.
-
Have the designated physician sign the form to validate the request.
To enhance the quality of your submission, double-check all entries for accuracy and completeness, paying particular attention to the medical justification provided.
Common Errors and How to Avoid Them When Submitting the Antirheumatic Agents Prior Authorization Review Request
When filling out the Antirheumatic Agents Prior Authorization Review Request, several common errors can lead to delays in processing. These mistakes may include missing signatures, incomplete fields, or inaccuracies in medical history. To avoid these pitfalls:
-
Thoroughly review the completed form before submission.
-
Ensure all required signatures are obtained, particularly from the physician.
-
Verify that the provided medical justification aligns with the patient's diagnosis.
Taking these precautions can significantly reduce the chances of processing delays and promote timely medication access for patients.
Submission Methods for the Antirheumatic Agents Prior Authorization Review Request
Submitting the Antirheumatic Agents Prior Authorization Review Request can be done through various methods, ensuring flexibility for healthcare providers. Available submission methods include:
-
Submitting the form via secure email.
-
Mailing a hard copy to the appropriate Pharmacy Management office.
-
Completing the form through an online portal for instant processing.
For optimal outcomes, it is recommended to choose a submission method that guarantees confirmation of receipt, thereby facilitating timely processing.
What Happens After You Submit the Antirheumatic Agents Prior Authorization Review Request
Upon submission of the Antirheumatic Agents Prior Authorization Review Request, it begins a review process that typically has a defined timeline. During this waiting period, it is essential to understand what to expect:
-
The review process generally takes several business days, depending on the complexity of the request.
-
Providers may need to follow up to check the status of their application.
-
Clear communication from the Pharmacy Management department will inform about the authorization decision.
Monitoring the submission status is important to ensure any requested additional information is promptly provided.
Security and Compliance When Handling the Antirheumatic Agents Prior Authorization Review Request
When dealing with the Antirheumatic Agents Prior Authorization Review Request, security and compliance are paramount. The handling of sensitive medical information incorporates various security measures:
-
Adherence to HIPAA regulations to protect patient privacy.
-
Use of secure platforms for document submission and storage.
-
Implementation of 256-bit encryption for data protection.
Understanding these security protocols ensures that patient information is safeguarded throughout the process.
Utilizing pdfFiller for the Antirheumatic Agents Prior Authorization Review Request
pdfFiller offers robust features that streamline the completion of the Antirheumatic Agents Prior Authorization Review Request. Users can benefit from:
-
Easy text editing and form filling capabilities.
-
eSigning options that allow for quick physician approval.
-
Enhanced security features to protect sensitive data during the form lifecycle.
Utilizing pdfFiller simplifies the entire process, making it more efficient and secure for healthcare providers and patients alike.
How to fill out the Prior Authorization Request
-
1.To access the Antirheumatic Agents Prior Authorization Review Request form on pdfFiller, visit the pdfFiller website and search for the form by name or category.
-
2.Once you find the form, click on it to open in the pdfFiller editor. Familiarize yourself with the layout and sections of the document.
-
3.Before filling in the form, gather all necessary patient information, including the patient's diagnosis, previous medications, and relevant medical justifications.
-
4.Begin entering the required information in the appropriate fields. Use the checkboxes for selections where applicable. Ensure accuracy to avoid delays.
-
5.If you need assistance, utilize pdfFiller's built-in help features or take advantage of the tutorial guides available on the platform.
-
6.Once all fields are completed, review the form carefully. Look for any missing information and double-check for accuracy.
-
7.After completing your review, finalize the form by signing it electronically within the pdfFiller platform, if required.
-
8.To submit the form, follow the instructions on pdfFiller for saving and downloading the file. You may also directly submit it from pdfFiller to the Pharmacy Management department as instructed.

Who is eligible to use the Antirheumatic Agents Prior Authorization Review Request form?
Healthcare providers, particularly physicians, are eligible to use this form to request prior authorization for antirheumatic medications needed for patient treatment.
What documents are required to complete this form?
Before filling out the form, you will need to gather patient-specific information, including the patient's diagnosis, a list of previous medications, and medical justifications for the requested treatment.
How do I submit the Antirheumatic Agents Prior Authorization Review Request form?
After completing the form on pdfFiller, you can submit it by downloading and emailing it to the Pharmacy Management department, or use pdfFiller's direct submission feature if available.
Are there any common mistakes to avoid when filling out this form?
Ensure all required fields are completed accurately. Common mistakes include neglecting to sign the form, leaving checkboxes unchecked, or providing incomplete patient information.
What is the typical processing time for prior authorization requests?
Processing times can vary by insurance provider, but generally expect notifications within 3 to 5 business days. Check directly with the insurance company for specific timelines.
Is notarization required for this form?
No, notarization is not required for the Antirheumatic Agents Prior Authorization Review Request form; however, it must be signed by the physician.
What happens if my prior authorization request is denied?
If denied, the pharmacy management department will typically provide a reason. You can appeal the decision by providing further documentation or clarification on the necessity of the medication.
Related Forms





Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.