Last updated on Mar 13, 2016

Get the free Appeal Form for Medicaid Denial
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
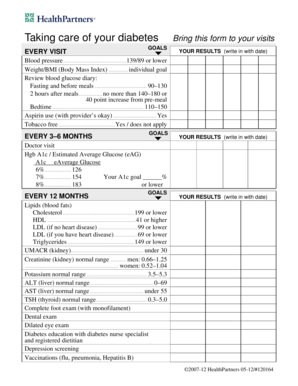
What is Medicaid Appeal Form
The Appeal Form for Medicaid Denial is a healthcare document used by Medicaid members in South Carolina to appeal a denial of coverage or service.
pdfFiller scores top ratings on review platforms
Who needs Medicaid Appeal Form?
Explore how professionals across industries use pdfFiller.

Medicaid Appeal Form is needed by:
-
Medicaid members facing a denial of coverage or services
-
Healthcare advocates assisting Medicaid users
-
Legal representatives handling Medicaid cases
-
Social workers supporting clients in healthcare appeals
-
Family members helping individuals with appeals
Comprehensive Guide to Medicaid Appeal Form
What is the Appeal Form for Medicaid Denial?
The Appeal Form for Medicaid Denial is integral for Medicaid members in South Carolina aiming to contest a denial of coverage or services. It allows users to formally present their case and seek a review of the decision made by Medicaid. Various types of denials can be appealed, including issues related to eligibility, service coverage, and payment disputes. Any Medicaid member or their authorized representative can utilize this form to initiate the appeals process within the state.
Purpose and Benefits of the Medicaid Denial Appeal Form
This form serves multiple key functions in the appeals process. Primarily, it provides a structured way for users to challenge a denial and express their concerns. Successful appeals can result in reinstated services, coverage, and financial support, ultimately impacting the well-being of the member and their family. Additionally, using the form can provide emotional support and a sense of empowerment to users facing the challenges of denial, reminding them that they have the right to appeal decisions that affect their healthcare.
Who Needs the Appeal Form for Medicaid Denial?
The appeal form is essential for individuals who have been denied Medicaid services, as well as for family members acting on their behalf. Users should consider filing an appeal if they receive a denial notice regarding their Medicaid application or service requests. Common scenarios that warrant the use of the appeal form include being denied coverage for necessary medical treatments, prescription drugs, or durable medical equipment.
Eligibility Criteria for Submitting the Medicaid Denial Appeal Form
In South Carolina, eligibility to submit the appeal form is generally extended to any Medicaid member who has received a denial notice. The types of denials that the form can address include those related to services not covered under Medicaid and decisions based on perceived ineligibility. It's important to note that there are strict time limits for submitting the appeal, typically required within 90 days of notification of the denial.
How to Fill Out the Appeal Form for Medicaid Denial
Filling out the appeal form involves several key steps:
-
Access the appeal form through the specified channels.
-
Complete all personal information fields, ensuring accuracy.
-
Clearly state the reason for the denial and any supporting arguments.
-
Gather any necessary supporting documentation, such as medical records and denial notices.
-
Review the completed form for completeness and accuracy before submission.
Pay special attention to the sections that require detailed explanations and documentation, as these can significantly affect the appeal outcome.
Review and Validation Checklist Before Submitting
To maximize the chances of a successful appeal, users should follow this checklist:
-
Verify all personal details are correct.
-
Ensure that the reason for appeal is clearly articulated.
-
Attach all required supporting documents.
-
Review the completed form for any errors or omissions.
-
Make sure to submit within the designated timeframe.
Accuracy and completeness are crucial in the submission process to avoid unnecessary delays or rejections.
Submission Methods for the Appeal Form for Medicaid Denial
The appeal form can be submitted through various methods:
-
Online submission via designated Medicaid portals.
-
Mailing the form to the appropriate Medicaid office.
-
In-person delivery at a local Medicaid office.
Be mindful of submission deadlines, as delays could impact the processing of the appeal. Retaining proof of submission is also essential for tracking and verification purposes.
What Happens After You Submit the Appeal Form?
Once the appeal form is submitted, the following steps typically occur:
-
The Medicaid office reviews the appeal and supporting documentation.
-
A decision is rendered, usually communicated to the member within a set timeframe.
-
If denied again, users have the option to further appeal or seek additional support.
Members are encouraged to check the status of their appeals periodically to stay informed about the proceedings.
Security and Compliance for the Medicaid Denial Appeal Form
When using pdfFiller for the appeal process, users benefit from robust security measures. pdfFiller employs 256-bit encryption and is compliant with HIPAA and privacy guidelines, ensuring that sensitive personal data remains protected throughout the appeal process. Users can confidently submit their information, knowing it is handled with the highest standards of data protection.
How pdfFiller Can Help with Your Medicaid Denial Appeal
pdfFiller offers an array of features that streamline the process of filling out the appeal form for Medicaid Denial. Users can easily edit, eSign, and manage forms directly on the platform, reducing the hassle associated with traditional methods. With a focus on user experience, pdfFiller helps ensure a seamless and efficient process for managing and submitting appeal forms.
How to fill out the Medicaid Appeal Form
-
1.Access pdfFiller and search for 'Appeal Form for Medicaid Denial.' Click on the form to open it in the editor.
-
2.Begin by reading the instructions carefully to understand what information is required.
-
3.Gather necessary personal information such as your Medicaid member ID, contact details, and specifics regarding the denial you are appealing.
-
4.Using pdfFiller's tools, fill in your personal information in the designated fields, ensuring accuracy for a smooth processing.
-
5.Clearly describe the nature of the denial and provide any additional context in the appropriate sections of the form.
-
6.Attach any required supporting documentation by using the upload feature in pdfFiller and ensure they are relevant to your appeal.
-
7.Once all fields are filled out, review your entries to check for mistakes or missing information.
-
8.Save your progress frequently to avoid losing information, and when ready, finalize the form.
-
9.To submit, either download the completed form in your desired format or use the submission feature provided by pdfFiller to send it directly.
-
10.Ensure that the completed form is submitted within 90 days of receiving the denial notice to avoid delays in processing your appeal.

What are the eligibility requirements for using this form?
To use the Appeal Form for Medicaid Denial, you must be a Medicaid member in South Carolina who has received a denial of coverage or service.
What is the deadline for submitting this appeal form?
You must submit the completed appeal form within 90 days of receiving the notice of denial to ensure consideration of your appeal.
How do I submit the Appeal Form for Medicaid Denial?
You can submit the completed form by downloading it and mailing it to the appropriate Medicaid office, or use pdfFiller's submission option for electronic submission.
What supporting documents are required with this form?
You should include any documentation that supports your case, such as medical records, letters from healthcare providers, and the denial notice from Medicaid.
What common mistakes should I avoid when filling out this form?
Common mistakes include forgetting to provide all required information, not reviewing for typos, and missing the 90-day submission deadline. Double-check everything before submitting.
How long does it take to process the appeal?
Processing times for appeals can vary depending on the complexity of the case, but typically you should expect a response within 30 to 90 days once submitted.
Who can assist me in filling out this appeal form?
You may seek assistance from healthcare advocates, social workers, legal representatives, or family members who are knowledgeable about the Medicaid appeal process.
Related Forms



Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.