Last updated on Mar 14, 2016
Get the free Claim Appeal Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
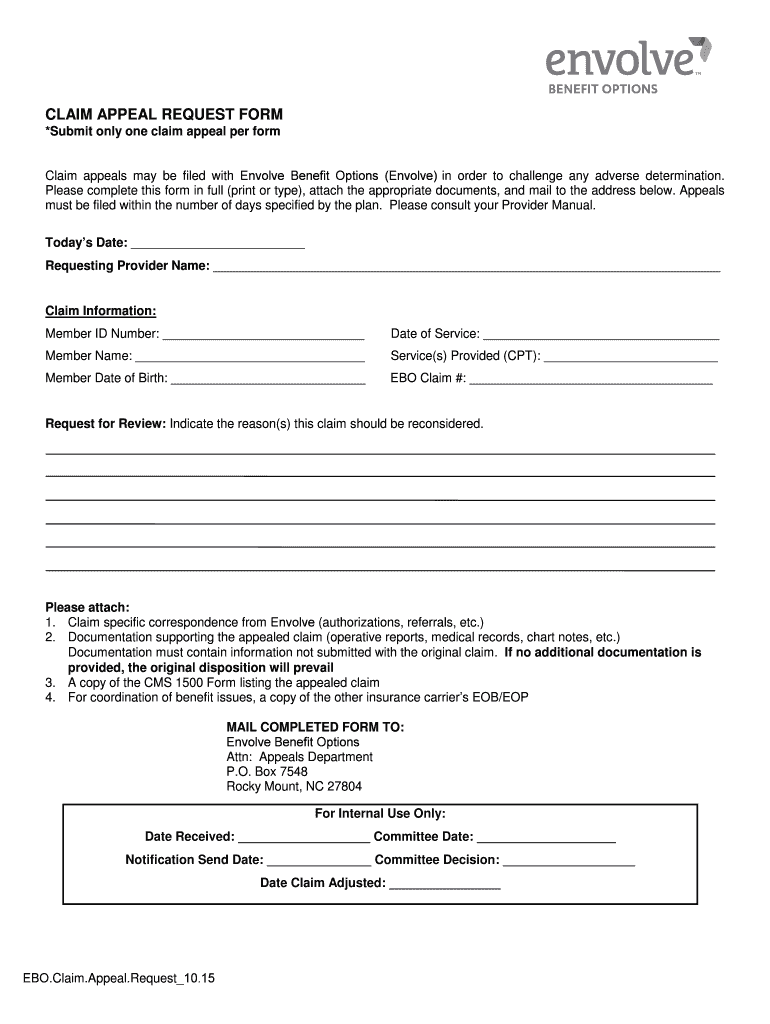
What is Claim Appeal Form
The Claim Appeal Request Form is a healthcare document used by members to challenge adverse determinations made by Envolve Benefit Options.
pdfFiller scores top ratings on review platforms
Who needs Claim Appeal Form?
Explore how professionals across industries use pdfFiller.

Claim Appeal Form is needed by:
-
Individuals seeking to appeal a healthcare claim decision
-
Healthcare providers assisting patients with claims
-
Legal representatives involved in healthcare disputes
-
Patients needing benefit options from Envolve
-
Insurance administrators managing claim appeals
Comprehensive Guide to Claim Appeal Form
What is the Claim Appeal Request Form?
The Claim Appeal Request Form serves a crucial function in the appeals process by enabling members to challenge adverse determinations made by Envolve Benefit Options. This form is specifically utilized to contest denied claims, ensuring that members have the ability to seek access to necessary healthcare services. Understanding its importance can significantly empower members navigating the complexities of healthcare claim appeals.
Purpose and Benefits of the Claim Appeal Request Form
The purpose of the Claim Appeal Request Form lies in its role as a critical tool for members looking to appeal adverse determinations, particularly in the healthcare sector. By utilizing this form, members can effectively contest denied claims, which ensures access to essential medical services. Additionally, it offers the advantage of providing a structured way to present supporting information, which can play a pivotal role in the success of an appeal.
Who Needs the Claim Appeal Request Form?
Various individuals and organizations may need to utilize the Claim Appeal Request Form. This includes members of Envolve Benefit Options who have had claims denied, as well as healthcare providers acting on behalf of their patients. To be eligible, members must ensure they meet the criteria set forth by Envolve Benefit Options, making this form relevant for a broad audience seeking resolution in their claims.
Key Features of the Claim Appeal Request Form
The Claim Appeal Request Form includes several key features that facilitate the appeals process. Essential components of the form comprise:
-
Member ID Number
-
Date of Service
-
Services Provided
-
Required attachments such as the CMS 1500 Form
These elements are critical for ensuring that claims are processed accurately and efficiently, enhancing the likelihood of a successful appeal.
How to Fill Out the Claim Appeal Request Form: A Step-by-Step Guide
Completing the Claim Appeal Request Form is straightforward when following these step-by-step instructions:
-
Start by filling out the 'Today’s Date' field.
-
Provide the 'Requesting Provider Name' accurately.
-
Ensure the 'Member ID Number' is correctly stated.
-
Detail the 'Date of Service' relevant to the claim.
-
List the 'Services Provided' comprehensively.
Be mindful of common errors such as omitting required fields or failing to attach necessary documentation, which can hinder the appeal process.
Submission Process for the Claim Appeal Request Form
To ensure your Claim Appeal Request Form is submitted correctly, consider the following submission methods:
-
Mail the completed form to the Appeals Department of Envolve Benefit Options in Rocky Mount, NC.
-
File electronically if such options are available through member portals.
Timeliness is critical; therefore, pay attention to submission deadlines to safeguard your right to appeal.
Consequences of Not Filing the Claim Appeal Request Form Timely
Failing to file the Claim Appeal Request Form by the specified deadlines can lead to significant consequences. Potential outcomes include the denial of the appeal or loss of rights to contest the claim. This can severely impact access to necessary healthcare services, underscoring the importance of timely filing.
Common Rejection Reasons for Claim Appeals and How to Avoid Them
Understanding common reasons for claim rejection can help members strengthen their appeals. Typical rejection reasons include:
-
Incomplete or inaccurate information on the form
-
Submission of insufficient supporting documentation
-
Missing deadlines for submission
By being aware of these common pitfalls, members can take proactive steps to enhance their chances of a successful appeal.
Security and Compliance When Using the Claim Appeal Request Form
When utilizing the Claim Appeal Request Form, data security and compliance are paramount. pdfFiller employs robust security measures, including 256-bit encryption, to protect sensitive information. Furthermore, adherence to HIPAA compliance ensures that users' health data is handled with the utmost privacy and security.
Get Started with the Claim Appeal Request Form Today!
pdfFiller simplifies the process of filling out and submitting the Claim Appeal Request Form. With cloud-based features and the ability to eSign documents, members can efficiently navigate the appeals process. Take advantage of these tools today to ensure your submission is as seamless as possible.
How to fill out the Claim Appeal Form
-
1.To begin, access pdfFiller and search for the Claim Appeal Request Form in the template library. Once found, click on the form to open it in the editing interface.
-
2.Use the intuitive tools provided by pdfFiller to navigate through the form. Click on each blank field to enter required information like your Member ID Number and Date of Service.
-
3.Prior to starting the form, gather all necessary information such as your Member ID Number, Dates of Service, service details, and any pertinent attachments like the CMS 1500 Form.
-
4.As you complete the form, carefully review each field to ensure accuracy. If any fields are not clear, refer to the explanations provided in the form for guidance.
-
5.After filling in all required fields, use pdfFiller’s preview option to review the completed form. Check for any errors or omissions before finalizing.
-
6.Once satisfied with the information, save your work using the 'Save' option. You can also choose to download the form in your preferred format or submit it directly through pdfFiller’s submission tools.

Who is eligible to use the Claim Appeal Request Form?
Any member of Envolve Benefit Options who has received an adverse determination regarding their healthcare claim can utilize this form to initiate an appeal.
What supporting documents are required with the form?
Along with the Claim Appeal Request Form, you need to attach the CMS 1500 Form and any other relevant supporting documentation to substantiate your appeal.
How do I submit the completed Claim Appeal Request Form?
After completing the form, it should be mailed to the Appeals Department in Rocky Mount, NC. Ensure you follow all submission instructions included on the form.
What is the deadline for submitting a claim appeal?
Claim appeals should generally be submitted within a specific time frame following the adverse decision. Ensure to check Envolve Benefit Options' guidelines for exact deadlines.
How long does it take to process a claim appeal?
Processing times for claim appeals can vary, but typically, you should expect a response within a few weeks after submission. Follow up if you don’t receive updates promptly.
What common mistakes should I avoid when completing the form?
Ensure all fields are filled completely and accurately. Common errors include missing Member ID Numbers, incorrect Dates of Service, and failing to attach required supporting documents.
Can healthcare providers submit this form on behalf of patients?
Yes, healthcare providers can assist patients in completing and submitting the Claim Appeal Request Form as long as they have the necessary consent and documentation.
Related Forms





Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.