Last updated on Mar 14, 2016
Get the free Member Claim Form for Out of Network Services
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
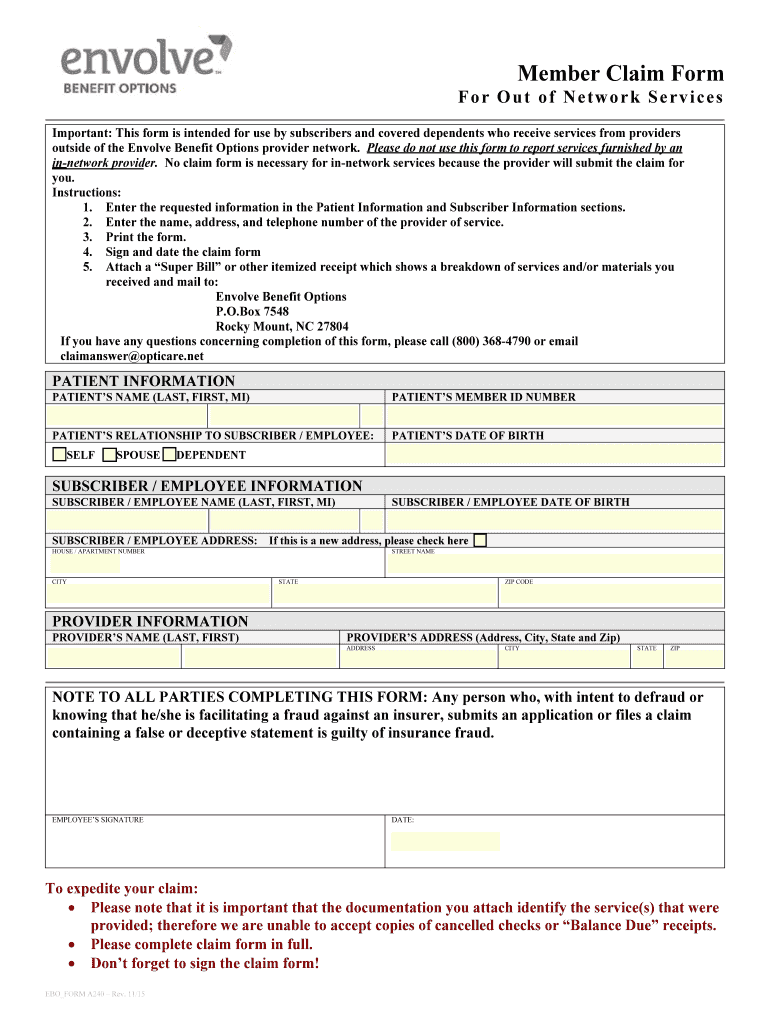
What is Out of Network Claim Form
The Member Claim Form for Out of Network Services is a medical billing document used by subscribers to request reimbursement for healthcare services received outside the Envolve Benefit Options network.
pdfFiller scores top ratings on review platforms
Who needs Out of Network Claim Form?
Explore how professionals across industries use pdfFiller.

Out of Network Claim Form is needed by:
-
Healthcare plan subscribers requiring reimbursement
-
Dependents covered under an Envolve health plan
-
Medical providers billing for out of network services
-
Administrative staff handling patient claims
-
Insurance agents assisting with claim submissions
Comprehensive Guide to Out of Network Claim Form
What is the Member Claim Form for Out of Network Services?
The Member Claim Form for Out of Network Services serves a crucial role in healthcare reimbursement, allowing subscribers and covered dependents to report medical services received from non-network providers. This form is essential for ensuring that claims are processed appropriately, enabling individuals to reclaim their medical expenses smoothly. The importance of accurately utilizing the out of network claim form cannot be understated, as it directly impacts the efficiency of reimbursements.
Purpose and Benefits of the Member Claim Form for Out of Network Services
Filing the Member Claim Form is significant for services rendered outside the established network. Properly utilizing this healthcare reimbursement form maximizes the likelihood of timely and adequate reimbursement for medical expenses. Envolve Benefit Options provides valuable support throughout this process, assisting users in navigating the intricacies of medical billing and ensuring compliance with requirements.
Who Needs the Member Claim Form for Out of Network Services?
This form is relevant for employees, subscribers, and their dependents when seeking reimbursement for out-of-network services. For instance, individuals who receive treatment from specialists not included in their healthcare network would need this form to file their claims. Eligibility criteria for completing the insurance claim form include being an enrolled member of the health plan and having incurred out-of-pocket expenses for healthcare services.
How to Fill Out the Member Claim Form for Out of Network Services (Step-by-Step)
To correctly fill out the Member Claim Form, follow these step-by-step instructions:
-
Provide subscriber information, including name, address, and member ID.
-
Enter details for the healthcare provider utilized, such as name and contact information.
-
Attach all necessary receipts for services rendered, ensuring they are itemized and clear.
-
Complete each field as accurately as possible to prevent delays in processing.
-
Review the form for accuracy and sign where indicated before submission.
Attention to detail can significantly reduce common mistakes that lead to claim rejections.
Required Documents and Supporting Materials for the Member Claim Form
To ensure a smooth filing process, you will need the following documents:
-
Itemized receipts from the healthcare provider for services received.
-
Any relevant medical records that substantiate the claims made.
-
The completed Member Claim Form, ensuring all required fields are filled.
Each document plays a critical role in your claim's success, so compiling them ahead of time can help streamline the process.
Submission Methods for the Member Claim Form for Out of Network Services
The Member Claim Form can be submitted via traditional mail directly to Envolve Benefit Options at their specified address. Alternatively, submitting digitally through pdfFiller offers a more efficient option, allowing for quick completion and electronic sharing of the form. Be mindful of submission deadlines and processing times to ensure your claims are handled promptly.
What Happens After You Submit the Member Claim Form?
After submission, users can expect a processing timeline where they may track their claims through designated channels. Multiple outcomes could result from this submission, including acceptance or rejection of the claims filed. It is crucial to understand common reasons for rejection, such as missing information or incorrect details, to address any issues promptly and refile if necessary.
Security and Compliance When Using the Member Claim Form
When completing the Member Claim Form, users can trust in the robust security measures employed by pdfFiller. With 256-bit encryption and adherence to HIPAA compliance, sensitive information is safeguarded throughout the entire process. This commitment to privacy and data protection ensures users can submit their documents without concern for unauthorized access.
Get Help with Your Member Claim Form Using pdfFiller
Utilizing pdfFiller can greatly enhance the efficiency of filling out the Member Claim Form. The platform offers capabilities such as editing, e-signing, and direct sharing, all accessible without needing downloads. Choosing pdfFiller ensures that users are leveraging a trusted and secure platform for their healthcare documentation needs.
Sample or Example of a Completed Member Claim Form for Out of Network Services
To assist users in navigating the completion of the Member Claim Form, a downloadable sample is available for review. This example highlights specific sections, demonstrating the type of information that should be included. By examining a real-world example, users can gain a clearer understanding of the necessary details for successful submission.
How to fill out the Out of Network Claim Form
-
1.To access the Member Claim Form for Out of Network Services on pdfFiller, visit the pdfFiller website and search for the form name in the search bar.
-
2.Once you locate the form, click on it to open the fillable PDF in pdfFiller's interface.
-
3.Familiarize yourself with the required fields; you will need to gather necessary information such as patient details, provider information, and itemized receipts before starting.
-
4.Carefully enter all required information into the designated fields; be sure to double-check that the subscriber's and patient's information are accurate.
-
5.Utilize pdfFiller's features to add your digital signature, as the completed form necessitates a signature for submission.
-
6.After completing the form, review all fields for accuracy and completeness to avoid common mistakes that can delay processing.
-
7.Finally, save your work and choose to download a copy of the form or submit it directly through pdfFiller's submission options.

Who is eligible to use the Member Claim Form for Out of Network Services?
The form is designed for subscribers and covered dependents who have utilized healthcare services from providers outside the Envolve Benefit Options network.
What supporting documents are required when submitting this form?
You must include an itemized receipt from the healthcare provider and any relevant patient information when submitting the Member Claim Form for Out of Network Services.
How should I submit the completed Member Claim Form?
Once completed, the form should be mailed to Envolve Benefit Options in Rocky Mount, NC. Ensure you keep a copy for your records.
Is there a deadline for submitting the Member Claim Form?
Although specific deadlines can vary, it's advisable to submit the form as soon as possible after receiving out of network services to avoid potential delays in reimbursement.
What are common mistakes to avoid when filling out the form?
Ensure all fields are filled out completely, particularly patient and provider information. Missing signatures or incorrect details can lead to processing delays.
How long does processing typically take after submission?
Processing times for claims can vary, but generally, you should expect a response within 30 days of submitting your completed Member Claim Form.
Can I fill out the Member Claim Form electronically?
Yes, you can complete the Member Claim Form electronically using pdfFiller before printing it for signature and submission.
Related Forms







Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.