Last updated on Mar 15, 2016
Get the free Medicaid Ostomy Products Provider Assistance Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Medicaid Ostomy Form
The Medicaid Ostomy Products Provider Assistance Form is a healthcare document used by Medicaid recipients to find providers of ostomy products.
pdfFiller scores top ratings on review platforms
Who needs Medicaid Ostomy Form?
Explore how professionals across industries use pdfFiller.

Medicaid Ostomy Form is needed by:
-
Medicaid recipients requiring ostomy products
-
Healthcare providers assisting patients with ostomy needs
-
Caregivers supporting Medicaid patients
-
Medical professionals seeking to facilitate ostomy care
-
Organizations helping with Medicaid health services
Comprehensive Guide to Medicaid Ostomy Form
Medicaid Ostomy Products Provider Assistance Form Overview
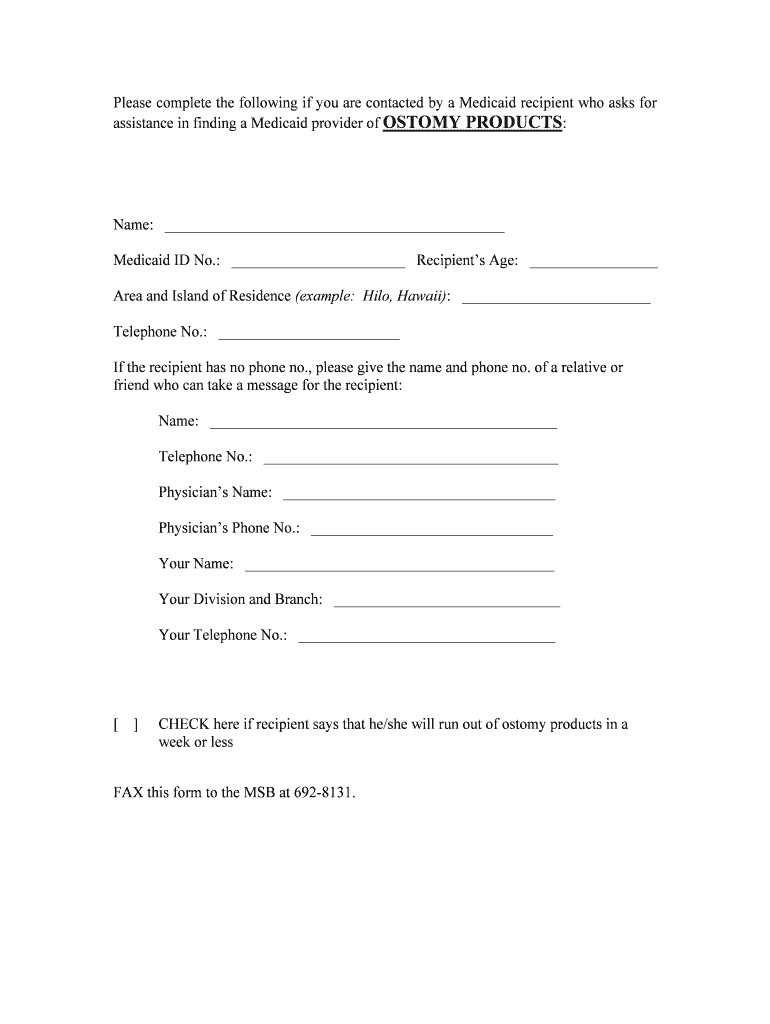
The Medicaid Ostomy Products Provider Assistance Form is designed to assist Medicaid recipients in locating suitable ostomy product providers. This essential document serves those needing assistance in managing their ostomy care, ensuring they receive the appropriate products to maintain their health and well-being. By utilizing the Medicaid provider form, users can streamline the process of finding reliable assistance for ostomy products.
Purpose and Benefits of the Medicaid Ostomy Products Provider Assistance Form
This form is critical for individuals navigating the complexities of managing their ostomy needs. One of the primary advantages is expedited assistance, allowing recipients to connect with approved Medicaid providers more efficiently. Additionally, the form helps secure the right care necessary to support proper health outcomes for those who rely on ostomy products.
Using the assistance form not only simplifies access to necessary resources but also enhances the overall quality of care for Medicaid recipients.
Key Features of the Medicaid Ostomy Products Provider Assistance Form
The Medicaid Ostomy Products Provider Assistance Form includes several noteworthy features that significantly aid users in completing their request. Key fields within the form include the recipient's Medicaid ID, contact details, and physician's information necessary for processing. Each submission incorporates a checkbox, indicating whether the recipient anticipates running low on ostomy supplies within a week, thereby prioritizing urgent needs.
These structured fields ensure that all relevant information is collected efficiently, enabling faster resolution and access to required ostomy products assistance.
Who Needs the Medicaid Ostomy Products Provider Assistance Form?
The target audience for the Medicaid Ostomy Products Provider Assistance Form primarily consists of qualified Medicaid recipients. Individuals who require assistance may include those recently diagnosed with conditions necessitating ostomy products or individuals experiencing changes in their care that demand new providers.
Situations prompting the need for this form often arise during transitions between care providers or when a recipient is unsure where to source their ostomy supplies.
How to Fill Out the Medicaid Ostomy Products Provider Assistance Form Online
Filling out the Medicaid Ostomy Products Provider Assistance Form online is a straightforward process that requires some preliminary information. Before starting, users should gather important details such as their Medicaid ID and physician’s contact information.
To efficiently complete each section of the form, users can follow these steps:
-
Access the pdfFiller platform for easy online form completion.
-
Input personal details including name, age, and residence.
-
Provide the Medicaid ID and physician’s information accurately.
-
Check the box if there is an upcoming product shortage.
-
Review all entries to ensure accuracy before final submission.
Utilizing pdfFiller offers an efficient way to fill out forms with features that enhance the overall experience.
Submission Methods for the Medicaid Ostomy Products Provider Assistance Form
Once the form is completed, recipients have various options for submission. These include online submission directly through the pdfFiller platform or mailing a physical copy to the appropriate Medicaid office. It is essential to be aware of any deadlines associated with these submission methods, as timely processing can vary.
Understanding the submission process ensures that users can navigate their options efficiently and receive prompt assistance.
What Happens After You Submit the Medicaid Ostomy Products Provider Assistance Form?
After submitting the Medicaid Ostomy Products Provider Assistance Form, users can expect a processing period during which their submission is reviewed. Typically, recipients will receive a notification confirming receipt of their application and information regarding what to anticipate next.
To stay informed, users can follow up on the status of their submissions through designated channels provided during the application process.
Security and Compliance for the Medicaid Ostomy Products Provider Assistance Form
Ensuring the security of sensitive information submitted via the Medicaid Ostomy Products Provider Assistance Form is paramount. pdfFiller implements robust security measures, including 256-bit encryption and adherence to HIPAA and GDPR compliance standards. This dedication to privacy and data protection safeguards personal health information shared during the form's completion.
Protecting users' data is not only a regulatory requirement but also a fundamental aspect of maintaining trust in the handling of medical documents.
Why Choose pdfFiller for Your Medicaid Ostomy Products Provider Assistance Form Needs
pdfFiller stands out as an ideal platform for managing the Medicaid Ostomy Products Provider Assistance Form with its array of features designed to enhance the user experience. The platform allows users to edit documents, eSign, and convert files between formats seamlessly, ensuring comprehensive support throughout the process.
User testimonials underline the effectiveness of pdfFiller in simplifying complex form submissions, encouraging others to utilize its capabilities for their assistance form OSTOMY needs.
How to fill out the Medicaid Ostomy Form
-
1.Access the Medicaid Ostomy Products Provider Assistance Form on pdfFiller by entering its name in the search bar or navigating to the healthcare forms section.
-
2.Open the form within pdfFiller's platform, ensuring you are in edit mode to fill out the necessary information.
-
3.Gather essential information before you start. This includes your full name, Medicaid ID number, age, address, telephone number, and your physician's contact details.
-
4.Find the labeled input fields in the form, click on each box to enter your information accordingly. Use the checkboxes to indicate if you're running low on ostomy products.
-
5.Review the filled form thoroughly to ensure all the fields are accurately completed, checking for any missed information or errors.
-
6.After reviewing, utilize pdfFiller's save and download options to keep a copy of your completed form. You can also submit the form directly through the platform if that's an available option.

Who is eligible to fill out the Medicaid Ostomy Products Provider Assistance Form?
Eligibility to fill out this form typically includes Medicaid recipients who need assistance in locating providers for ostomy products.
What information do I need to complete the form?
You will need to provide your name, Medicaid ID, age, address, telephone number, your physician's details, and the contact information of the person assisting you.
Can I submit the form online?
Yes, if you are using pdfFiller, you can submit the completed form directly through the platform, ensuring all fields are filled in correctly.
Is there a deadline for submitting the form?
While specific deadlines may not be stated, it is advisable to submit the form promptly, especially if you are running low on ostomy products.
What common mistakes should I avoid while filling out the form?
Common mistakes include leaving required fields blank, providing incorrect information, or failing to indicate urgent needs using the checkbox provided.
How long does it take to process the form?
Processing times can vary, but typically, once submitted, allow a few business days for providers to review and respond to your assistance request.
Are there any fees associated with submitting this form?
No fees are typically associated with filling out and submitting the Medicaid Ostomy Products Provider Assistance Form, as it is geared towards assistance for Medicaid recipients.
Related Forms



Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.