Last updated on Mar 16, 2016

Get the free ORBACTIV Physician Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
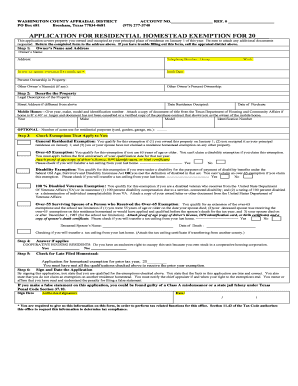
What is ORBACTIV Request Form
The ORBACTIV Physician Request Form is a patient assistance program document used by physicians to request insurance verification and pre-authorization for ORBACTIV (oritavancin).
pdfFiller scores top ratings on review platforms
Who needs ORBACTIV Request Form?
Explore how professionals across industries use pdfFiller.

ORBACTIV Request Form is needed by:
-
Physicians seeking insurance verification for patients
-
Healthcare providers managing ORBACTIV treatments
-
Medical practices involved in patient assistance programs
-
Billing departments handling pre-authorization requests
-
Patients requiring ORBACTIV treatment support
Comprehensive Guide to ORBACTIV Request Form
What is the ORBACTIV Physician Request Form?
The ORBACTIV Physician Request Form is designed for healthcare providers to facilitate the process of requesting ORBACTIV (oritavancin) patient assistance, insurance verification, and pre-authorization. This form plays a crucial role in ensuring patients receive timely care by streamlining communication between physicians and insurers. Completing the ORBACTIV Physician Request Form accurately is imperative for obtaining necessary treatments and support.
Purpose and Benefits of the ORBACTIV Physician Request Form
The primary purpose of the ORBACTIV Physician Request Form is to aid in the effective verification of insurance coverage and the pre-authorization process. By utilizing this form, healthcare providers can enhance the efficiency of obtaining necessary treatments for their patients. The benefits of this form include:
-
Streamlined communication between healthcare providers and insurance companies.
-
Improved chances for timely treatment authorizations.
-
Clear documentation for insurance verification and record-keeping.
Key Features of the ORBACTIV Physician Request Form
The ORBACTIV Physician Request Form includes several key features that ensure thorough completion and compliance, including:
-
Fillable fields and checkboxes for easy input.
-
A required physician signature and date to validate the request.
-
Sections that capture essential details such as physician information, patient data, insurance specifics, and treatment settings.
Who Needs the ORBACTIV Physician Request Form?
Various stakeholders are involved in the process that necessitates the use of the ORBACTIV Physician Request Form. Primary users include:
-
Physicians who need to initiate treatment requests.
-
Healthcare providers assisting patients with insurance processes.
-
Patients who can benefit from timely access to ORBACTIV treatments through effective use of the form.
This form is critical in scenarios requiring prior authorization or assistance from insurance providers.
How to Fill Out the ORBACTIV Physician Request Form (Step-by-Step)
To successfully complete the ORBACTIV Physician Request Form, follow these detailed steps:
-
Fill in the physician's details, including name, contact information, and licensing information.
-
Provide patient information, ensuring accuracy in details such as date of birth and medical history.
-
Complete the insurance information section, noting the provider and policy details.
-
Fill out the treatment setting and any additional requirements stipulated in the form.
-
Sign and date the form to validate the submission.
Be mindful of common errors, such as leaving fields blank or misentering numbers, to ensure a smooth submission process.
Review and Validation Checklist for the ORBACTIV Physician Request Form
Before submitting the ORBACTIV Physician Request Form, it’s important to perform a thorough review. Key points to check include:
-
Ensuring all fields are filled out completely, with no blanks.
-
Validating the accuracy of the physician and patient details.
-
Confirming the signature and date are present.
Taking the time to double-check these details can prevent common validation errors that may delay treatment.
How to Submit the ORBACTIV Physician Request Form
Submitting the ORBACTIV Physician Request Form can be accomplished through several methods:
-
Online submission through designated healthcare provider platforms or portals.
-
Email submission to the appropriate insurer or healthcare office.
-
Mailing a physical copy to ensure delivery to necessary parties.
Tracking confirmation after the submission is vital to ensure the request is processed effectively.
Security and Compliance for Handling the ORBACTIV Physician Request Form
Handling sensitive patient information with the utmost security is paramount. The ORBACTIV Physician Request Form adheres to strict compliance protocols, including:
-
HIPAA and GDPR guidelines for patient data protection.
-
Using 256-bit encryption to safeguard all submitted information.
-
Ensuring that only authorized individuals have access to sensitive data.
Utilizing pdfFiller for the ORBACTIV Physician Request Form
pdfFiller simplifies the process of completing and managing the ORBACTIV Physician Request Form. The platform offers numerous benefits:
-
Enabling easy editing and input of necessary information.
-
Providing options for eSigning and securely managing documents.
-
Making it convenient to create, fill out, and submit the form for maximum efficiency.
Sample Completed ORBACTIV Physician Request Form
Reviewing a sample completed ORBACTIV Physician Request Form can provide valuable insight into how to accurately fill out your own request. Key areas typically highlighted include:
-
Correctly input patient demographic information.
-
Completion of insurance details.
-
Signature and date properly executed by the physician.
How to fill out the ORBACTIV Request Form
-
1.Access pdfFiller and log in to your account. If you do not have an account, create one to begin.
-
2.Locate the ORBACTIV Physician Request Form by using the search function on the pdfFiller homepage.
-
3.Once found, click to open the form in pdfFiller's editor.
-
4.Review the form's fields, which may include sections for your personal details, patient information, insurance specifics, and treatment details.
-
5.Before filling out the form, gather all necessary information including patient medical records, insurance carrier details, and treatment authorization requirements.
-
6.Begin filling in the required fields by selecting and typing your information into the designated areas within the pdfFiller interface.
-
7.Use checkboxes for any options that require selection, ensuring all are accurately marked as applicable.
-
8.Once all fields are completed, carefully review each section for accuracy. Double-check that all information corresponds to the patient and insurance correctly.
-
9.Sign and date the form where necessary. Be aware that your signature certifies the accuracy of the information provided.
-
10.After finalizing the form, proceed to save it within your pdfFiller account or download a copy to your device.
-
11.To submit the form, check for submission options, which may include emailing it directly from pdfFiller or downloading for manual submission to the appropriate entity.

Who is eligible to use the ORBACTIV Physician Request Form?
The ORBACTIV Physician Request Form is designed for licensed physicians who are requesting insurance verification or pre-authorization for their patients receiving ORBACTIV treatment.
What information do I need to complete the form?
To complete the ORBACTIV Physician Request Form, you will need patient personal information, insurance details, and treatment-specific information, including dosage and administration details of ORBACTIV.
How do I submit the ORBACTIV Physician Request Form?
You can submit the ORBACTIV Physician Request Form either by emailing it directly from pdfFiller after completion or by downloading it and submitting it via your preferred method, ensuring it reaches the designated insurance company or provider.
Are there deadlines for submitting the ORBACTIV request form?
While the form itself does not impose deadlines, it is advisable to submit the ORBACTIV Physician Request Form as soon as possible to ensure timely insurance processing and treatment initiation for the patient.
What common mistakes should I avoid when filling out the form?
Common mistakes include leaving fields blank, providing incorrect insurance details, or failing to sign and date the form. Always double-check for accuracy to prevent delays.
How long does it take to process the ORBACTIV request form?
Processing times for the ORBACTIV Physician Request Form may vary based on the insurance provider. Typically, you should allow for several business days for approval or additional requests for information.
Do I need any supporting documents with the form?
Yes, it is often helpful to include any relevant supporting documents such as patient medical records or previous treatment information to facilitate the insurance verification process.
Related Forms






Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.