Last updated on Mar 16, 2016
Get the free Provider Request for Member Reassignment
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Member Reassignment Request
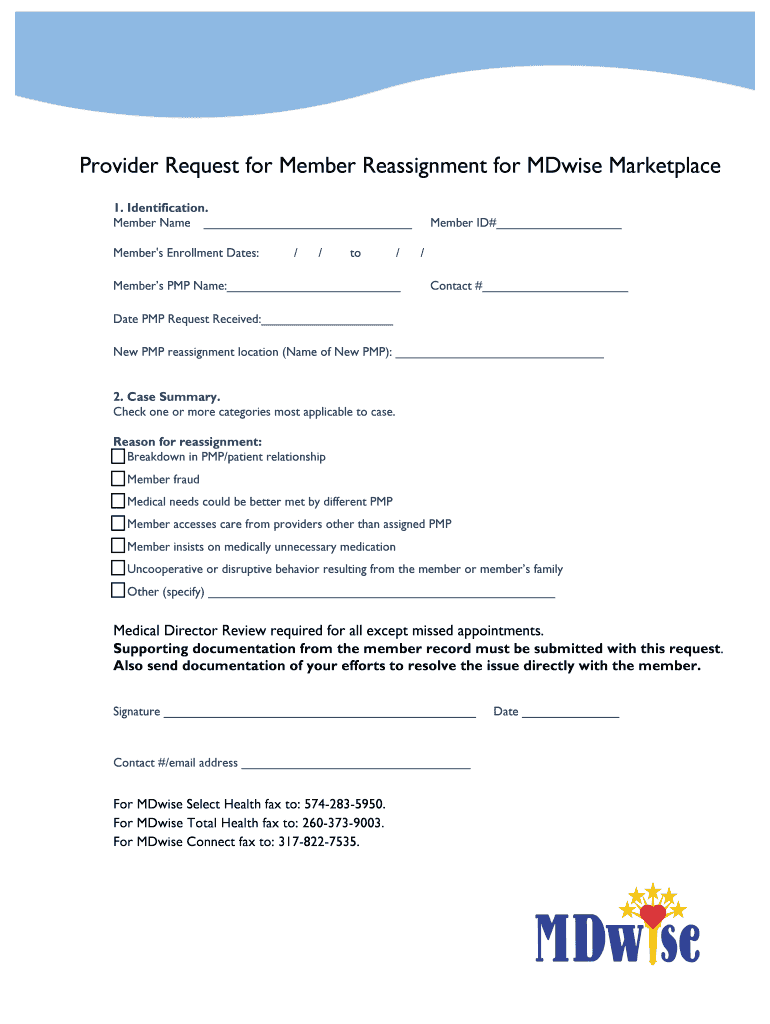
The Provider Request for Member Reassignment form is a healthcare document used by providers to request the assignment of a member to a new Primary Medical Provider (PMP) within the MDwise Marketplace.
pdfFiller scores top ratings on review platforms
Who needs Member Reassignment Request?
Explore how professionals across industries use pdfFiller.

Member Reassignment Request is needed by:
-
Healthcare providers needing to change a member's PMP.
-
Administrators managing member assignments in healthcare systems.
-
Patients seeking a different provider for their medical needs.
-
Insurance companies facilitating member reassignments.
-
Medical offices requiring updated assignment documentation.
Comprehensive Guide to Member Reassignment Request
What is the Provider Request for Member Reassignment?
The Provider Request for Member Reassignment is a crucial form used by healthcare providers to request the reassignment of a member to a new Primary Medical Provider (PMP). This request is essential for ensuring that the medical needs of patients are adequately met. Timely reassignment can significantly impact the quality of care, making it imperative for providers to understand the function of this form in the MDwise Marketplace.
Purpose and Benefits of Using the Provider Request for Member Reassignment Form
The purpose of this form is to streamline the reassignment process, thereby enhancing patient care and strengthening provider relationships. By utilizing the member reassignment form, providers can efficiently address any concerns that may arise with current PMPs. Additionally, pdfFiller offers a convenient platform for completing and submitting the form, simplifying the administrative tasks associated with healthcare provider requests.
Who Needs the Provider Request for Member Reassignment?
This form is intended for various types of healthcare providers, including physicians and specialists who may find it necessary to request a PMP reassignment. Situations such as dissatisfaction with the care provided by a current PMP or changes in a patient's medical needs often necessitate the use of this form. Understanding who requires the healthcare provider reassignment is key for both providers and patients to navigate the system efficiently.
How to Fill Out the Provider Request for Member Reassignment Online (Step-by-Step)
To complete the Provider Request for Member Reassignment through pdfFiller, follow these steps:
-
Access the MDwise Marketplace form on pdfFiller's platform.
-
Enter the patient's identification details in the specified fields.
-
Provide the reasons for the reassignment clearly in the designated section.
-
Attach any necessary supporting documentation for your request.
-
Review all information for accuracy before finalizing.
-
Sign the form electronically to complete the submission process.
Common Errors and How to Avoid Them When Submitting the Provider Request for Member Reassignment
Submitting the form accurately is vital to prevent delays or rejections. Common errors include:
-
Missing provider signatures, which can invalidate the submission.
-
Incorrect member information such as mismatched identification details.
-
Failure to attach required supporting documents.
Double-checking each field before submission can help avoid these pitfalls.
Submitting Your Provider Request for Member Reassignment
When you're ready to submit your Provider Request for Member Reassignment, consider the following points:
-
The preferred method of submission is online via pdfFiller for immediate processing.
-
Alternative submission methods include mailing the completed form.
-
Be aware of any applicable fees, submission deadlines, and processing times associated with your request.
What Happens After You Submit Your Provider Request for Member Reassignment?
After submission, you have options to track the status of your reassignment request. This can often be done through the platform used for submission. Common reasons for delays or rejections can include:
-
Inadequate supporting documentation.
-
Mismatched information on the form.
Addressing these issues promptly can help resolve any barriers to processing your request.
Security and Compliance for the Provider Request for Member Reassignment
Ensuring the security and compliance of sensitive data is paramount when handling the Provider Request for Member Reassignment. pdfFiller implements robust security measures, including:
-
256-bit encryption to protect user data.
-
Compliance with HIPAA regulations to safeguard patient information.
Maintaining privacy and data protection is essential during the reassignment process.
Utilizing pdfFiller for Your Provider Request for Member Reassignment
pdfFiller greatly simplifies the process of completing the Provider Request for Member Reassignment. Its cloud-based features allow for easy access, editing, eSigning, and sharing of documents. Providers can benefit from using pdfFiller by enjoying the convenience of managing forms from any device, enhancing their overall efficiency in handling member reassignment requests.
Sample of a Completed Provider Request for Member Reassignment
To assist users in understanding the completion of the form, a sample filled-out Provider Request for Member Reassignment is available. This example illustrates key sections of the form, providing clarity on necessary details and best practices for submission.
How to fill out the Member Reassignment Request
-
1.Access pdfFiller and search for the 'Provider Request for Member Reassignment' form using the search bar on the homepage.
-
2.Once the form appears, click on it to open it in the pdfFiller editing view.
-
3.Ensure you have all identification details, reasons for reassignment, and any supporting documents prepared before you start filling out the form.
-
4.Begin completing the form by filling in the blank fields with the required information, such as member details and existing PMP information.
-
5.Use the checkboxes to indicate the appropriate reasons for the reassignment, ensuring to read each option carefully.
-
6.When you finish filling out the fields, review each entry for accuracy and completeness to avoid common mistakes.
-
7.Once reviewed, navigate to the signature section and add your electronic signature as the provider.
-
8.After signing, take a moment to review the entire document once more to confirm all information is correct.
-
9.To save your completed form, click on the 'Save' button, or download it directly to your device using the 'Download' option available.
-
10.You can also submit the form directly through pdfFiller if your organization has set that up. Ensure you follow any additional submission instructions as required.

Who is eligible to use the Provider Request for Member Reassignment form?
Healthcare providers who need to request reassignments for members to new Primary Medical Providers within the MDwise Marketplace are eligible to use this form.
What is the process for submitting the form?
The form can be submitted digitally through pdfFiller or printed and sent via postal mail, depending on your organization's submission protocols.
What supporting documents do I need to provide?
You will need to include identification details and any relevant documentation that supports the request for reassignment, such as member history or specific medical needs.
How can I ensure my form is filled out correctly?
Review all provided instructions on the form carefully, double-check your entries for accuracy, and make sure to provide all required signatures and supporting documents.
Are there any deadlines for submitting this form?
While specific deadlines may vary by organization, it's crucial to submit the form as soon as the need for reassignment arises to ensure timely changes in care.
What should I do if I encounter issues while filling out the form on pdfFiller?
If you encounter any issues, refer to pdfFiller's help section for troubleshooting guides or contact their customer support for assistance with the platform.
How long does it take for the reassignment to be processed?
Processing times can vary, but typically, reassignments are reviewed and completed within a few business days once all necessary documents are submitted.
Related Forms





Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.