Last updated on Mar 17, 2016
Get the free Authorization to Release Medical Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Medical Release Form
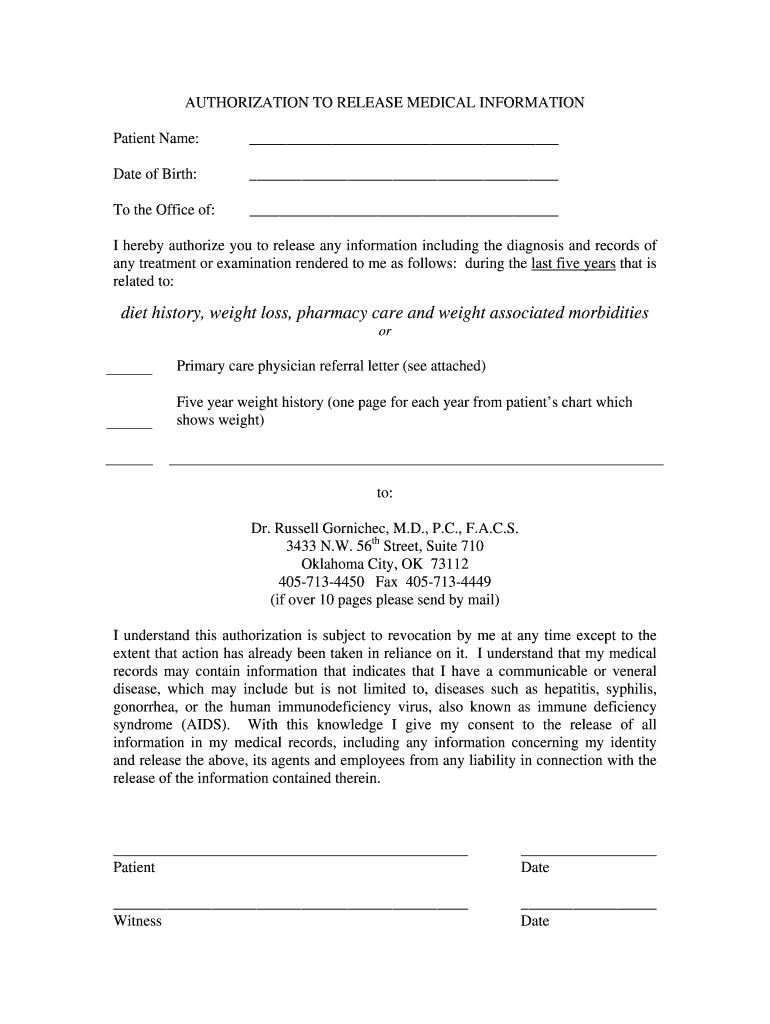
The Authorization to Release Medical Information is a medical records release form used by patients to grant permission for the dissemination of their health records.
pdfFiller scores top ratings on review platforms
Who needs Medical Release Form?
Explore how professionals across industries use pdfFiller.

Medical Release Form is needed by:
-
Patients seeking to share medical records with new healthcare providers.
-
Physicians needing access to a patient's medical history for treatment.
-
Pharmacies requiring approval to share medication records.
-
Health organizations managing patient diet and weight-related care.
-
Witnesses verifying the patient's authorization signature.
Comprehensive Guide to Medical Release Form
What is the Authorization to Release Medical Information?
The Authorization to Release Medical Information form is crucial in the healthcare context, specifically for patients seeking to manage their medical records. It allows patients to grant permission for the distribution of their medical information pertaining to weight loss, pharmacy care, and detailed diet history. This form is directed towards healthcare providers in Oklahoma, ensuring a structured protocol for sharing sensitive data. By utilizing this medical release form, patients can effectively streamline their healthcare experience.
Benefits of Using the Authorization to Release Medical Information
Utilizing the Authorization to Release Medical Information offers significant advantages for patients. It enhances access to medical records, which is vital for effective healthcare management and communication between patients and healthcare providers. Granting access to medical records can lead to improved treatment options, especially in managing weight-related morbidities and conditions. By using this patient authorization form, individuals can ensure they are fully supported in their health journeys.
Key Features of the Authorization to Release Medical Information Form
The Authorization to Release Medical Information form contains several essential features designed to facilitate its use. Key fillable fields include:
-
Patient Name
-
Date of Birth
-
Signature lines for both the patient and witness
This form also requires a five-year weight history and a referral letter from a physician, which further aids in weight loss management. Both patient and witness signatures are necessary to validate the form and ensure compliance with medical guidelines in Oklahoma.
Who Should Fill Out the Authorization to Release Medical Information?
This authorization form should be filled out by patients who need to share their medical information for various purposes. Patients play an integral role in completing this form, while witnesses are essential for validating the process. Authorization is particularly necessary for healthcare providers when dealing with sensitive medical information. The eligibility criteria for completing the form are often determined by specific treatment goals, such as those related to weight loss management.
Step-by-Step: How to Fill Out the Authorization to Release Medical Information Online
To fill out the Authorization to Release Medical Information online using pdfFiller, follow these steps:
-
Access the pdfFiller platform from your web browser.
-
Locate the form template for Authorization to Release Medical Information.
-
Fill in each required field accurately, including personal information and medical details.
-
Review your entries to ensure all information is correct.
-
Obtain signatures from both the patient and witness.
-
Submit the completed form based on the chosen submission method.
Before you finalize your submission, check for information accuracy and ensure all necessary signatures are included.
Submission Process for the Authorization to Release Medical Information
Submitting the Authorization to Release Medical Information can be done through various channels. You may choose electronic submission or in-person delivery, depending on your preference and provider guidelines. Keep in mind any state-specific requirements that may necessitate additional documentation. After submission, both patients and providers should track the status to ensure that the request is processed efficiently.
Security and Compliance with the Authorization to Release Medical Information
Security is paramount when handling sensitive medical data, and robust measures are implemented to protect personal information. This includes compliance with legal standards such as HIPAA and GDPR, which govern patient information protection. Additionally, record retention requirements are established to maintain privacy and ensure accountability in handling health information.
Common Mistakes to Avoid When Filling Out the Authorization to Release Medical Information
To ensure the successful completion of the Authorization to Release Medical Information, it's important to avoid common mistakes that may delay processing. Patients should be cautious of:
-
Leaving fields incomplete
-
Failing to obtain necessary signatures from witnesses
Double-checking submitted information for accuracy is essential, and validating witness signatures when applicable can prevent potential issues during submission.
Examples and Templates for the Authorization to Release Medical Information
Visual references can enhance understanding of the Authorization to Release Medical Information. Users may access downloadable samples of completed authorization forms for guidance. Variations of this form may exist for different contexts, and pdfFiller offers customization options for users to tailor their forms according to specific needs.
Start Using pdfFiller for Your Authorization to Release Medical Information
pdfFiller streamlines the process of completing the Authorization to Release Medical Information form. With its user-friendly interface, creating and filling out forms becomes efficient and straightforward. Users can also explore additional resources available through pdfFiller for other healthcare-related documentation, facilitating a comprehensive approach to managing medical records securely.
How to fill out the Medical Release Form
-
1.Access the Authorization to Release Medical Information form by visiting pdfFiller and searching for the form using its name.
-
2.Once you find the form, click on it to open it in the pdfFiller editor.
-
3.Before starting, gather required information such as the patient's full name, date of birth, and any relevant healthcare provider details.
-
4.Begin filling in the fields in the document, entering the patient's name, date of birth, and other necessary information as prompted in each field.
-
5.Utilize pdfFiller’s tools to add your signature in the designated area and ensure the witness also has a chance to sign where indicated.
-
6.Once all fields are completed, review the entire form for accuracy, ensuring all necessary information is filled in correctly and signatures are added.
-
7.After reviewing, choose the option to save or download the completed form directly from pdfFiller for your records.
-
8.If you plan to submit the form electronically, follow the provided submission options on pdfFiller, ensuring any additional documents are attached as required.

Who is eligible to use the Authorization to Release Medical Information form?
The form is designed for patients in Oklahoma who want to share their medical records. Anyone with legal authority to grant access to their own medical history can complete this form.
What information do I need to fill out this form?
You will need the patient's full name, date of birth, and details about the healthcare providers who need access to the medical records. Ensure you have accurate contact information on hand.
Is there a deadline for submitting this form?
While the form itself does not have a strict deadline, it’s important to submit it as soon as possible to ensure timely access to medical records when needed.
Can I complete this form electronically?
Yes, the Authorization to Release Medical Information can be completed and submitted electronically via pdfFiller, which allows you to fill, sign, and share the form online.
What should I do if I make a mistake on the form?
If you notice an error after you have filled out the form, simply correct it directly in pdfFiller before saving or submitting it. Always review all entries carefully for accuracy.
Does the form require notarization?
No, the Authorization to Release Medical Information does not require notarization, but it does need to be signed by both the patient and a witness.
How can I save or submit the completed form?
After completing the form in pdfFiller, you can save it to your device or submit it directly to the designated recipient via email or online submission, depending on the provider's requirements.
Related Forms






Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.