Last updated on Mar 17, 2016
Get the free Health Net Medical Plan Change Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
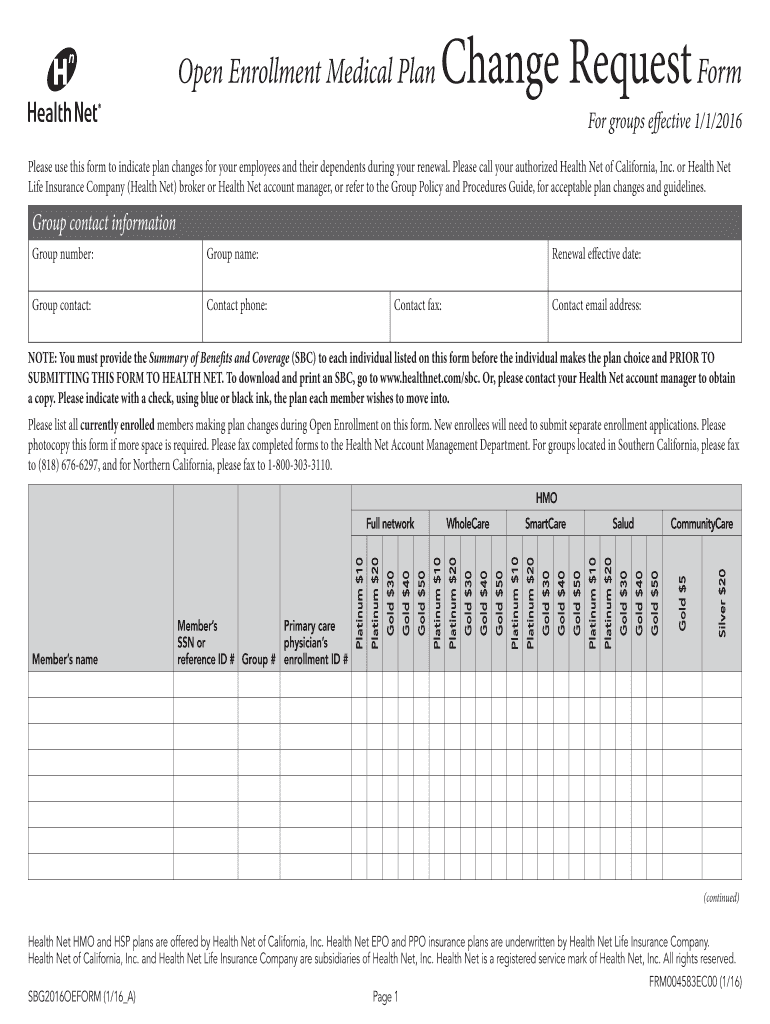
What is Medical Plan Change Form
The Health Net Medical Plan Change Request Form is a healthcare document used by group administrators in California to request changes in medical plans for employees and their dependents.
pdfFiller scores top ratings on review platforms
Who needs Medical Plan Change Form?
Explore how professionals across industries use pdfFiller.

Medical Plan Change Form is needed by:
-
Group administrators managing employee medical plans
-
HR personnel in California-based organizations
-
Employees looking to change their health insurance coverage
-
Dependents who need to update their insurance information
-
Insurance brokers assisting clients with plan changes
-
Account managers handling group health plans
Comprehensive Guide to Medical Plan Change Form
What is the Health Net Medical Plan Change Request Form?
The Health Net Medical Plan Change Request Form serves as a vital tool for group administrators in California, enabling them to request changes to employee health coverage. This form is designed to assist with critical shifts during plan renewals, ensuring that all necessary adjustments are properly documented. It captures essential information including group contact details and member specifics, highlighting its importance in maintaining accurate employee records.
Key details required on the form include group number, renewal effective date, and specific plan selections. Accurate completion of this form is crucial as it directly impacts employee coverage and compliance with California health insurance regulations.
Purpose and Benefits of the Health Net Medical Plan Change Request Form
Utilizing the Health Net Medical Plan Change Request Form is essential, especially during the open enrollment or renewal period. This form aids in streamlining the process of implementing plan changes for employees and their dependents, thus enhancing the overall administration experience.
By ensuring compliance with regulatory requirements, using this form can lead to improved employee satisfaction and confidence in coverage options. Additionally, it helps organizations maintain efficient operations and timely updates to health insurance plans.
Who Needs the Health Net Medical Plan Change Request Form?
The primary users of the Health Net Medical Plan Change Request Form include group contacts and administrators responsible for managing employee benefits. Scenarios necessitating the use of this form range from changes in coverage levels to updates in employer-provided options.
Particularly, groups operating within California are eligible to take advantage of this form, making it a critical resource for local organizations to ensure their health plan offerings are current and compliant.
How to Fill Out the Health Net Medical Plan Change Request Form Online
Filling out the Health Net Medical Plan Change Request Form online via pdfFiller is a straightforward process. Begin by accessing the form, where you’ll encounter several fillable fields such as 'Group number,' 'Renewal effective date,' and other pertinent information required for submission.
To ensure accuracy and completeness, check each entry before finalizing the form. Pay special attention to critical fields, and utilize any available tips or guides provided by pdfFiller to enhance the filling experience.
Required Documents for Submission of the Health Net Medical Plan Change Request Form
When submitting the Health Net Medical Plan Change Request Form, it’s crucial to include supporting materials to facilitate successful processing. Key supporting documents include the Summary of Benefits and Coverage (SBC) and any other relevant evidence of coverage changes.
To help streamline your submission, consider using a pre-filing checklist that lists necessary documents for gathering before you begin the form. This preparation can prevent delays and ensure all prerequisites are in place.
Submission Methods for the Health Net Medical Plan Change Request Form
After completing the Health Net Medical Plan Change Request Form, users have several submission methods available. You can choose to fax the form directly to the Health Net Account Management Department or send digital versions using platforms like pdfFiller.
Be aware that specific timelines for processing and potential fees may apply, depending on the submission method selected. Keeping this in mind will help ensure a smoother transition during the submission phase.
Common Errors and How to Avoid Them When Filing the Form
When completing the Health Net Medical Plan Change Request Form, users often encounter common errors that can result in rejections or processing delays. Frequent mistakes include entering incorrect group numbers or failing to provide all required member details.
To avoid these pitfalls, create a review and validation checklist. Key items to double-check include completeness of all fields, accuracy of contact information, and the inclusion of necessary supporting documents.
Security and Compliance When Using the Health Net Medical Plan Change Request Form
Security is paramount when submitting sensitive documents like the Health Net Medical Plan Change Request Form. pdfFiller utilizes 256-bit encryption and adheres to compliance standards including HIPAA and GDPR, ensuring user data is protected throughout the processing stages.
By using pdfFiller, users can trust that their documents are handled securely, instilling confidence in the privacy and data protection measures employed during document management.
What Happens After You Submit the Health Net Medical Plan Change Request Form?
Once you submit the Health Net Medical Plan Change Request Form, you should expect a confirmation of receipt from Health Net. This step is crucial, as it provides reassurance that your request is being processed.
If additional information is requested, be prepared to respond promptly. Additionally, you can check the status of your application through Health Net’s available channels to stay informed on any updates or required actions post-submission.
Maximize Your Experience with the Health Net Medical Plan Change Request Form Using pdfFiller
To enhance your experience with the Health Net Medical Plan Change Request Form, make the most of pdfFiller's robust editing and filling capabilities. The platform simplifies the creation, filling, and eSigning processes, allowing you to manage healthcare forms efficiently and securely.
Utilizing pdfFiller not only streamlines your documentation process but also ensures your health-related forms are completed correctly and processed in a timely manner, benefitting both administrators and employees alike.
How to fill out the Medical Plan Change Form
-
1.To begin, visit pdfFiller and log into your account or create a new one if necessary. Use the search function to find the 'Health Net Medical Plan Change Request Form'.
-
2.Once the form is displayed, click to open it. Familiarize yourself with the layout and available fields that you are required to fill in.
-
3.Before completing the form, gather all necessary information such as your group number, group name, and the renewal effective date. Additionally, have your group contact details and selected plans ready for input.
-
4.Use the toolbars provided by pdfFiller to navigate through the fillable fields. Click on each field to enter relevant data. Utilize the checkboxes for plan selection according to your preferences.
-
5.Once all fields are filled accurately, take a moment to review your entries. Ensure that all contact information is correct and all required sections are completed.
-
6.pdfFiller provides options to save your progress or finalize the document. After reviewing, choose the option to save your completed form locally or download it directly in your desired format.
-
7.If you are ready to submit, follow the instructions to fax the completed form to the Health Net Account Management Department as per the submission requirement.

Who is eligible to use the Health Net Medical Plan Change Request Form?
The form is primarily for group administrators in California managing employee health plans. Employees and their dependents needing plan changes may also require this form.
What is the deadline for submitting the Health Net Medical Plan Change Request Form?
Submissions should typically be made during the renewal period. Check with your Health Net representative for specific deadlines to ensure timely processing.
How do I submit the completed form?
You must fax the completed Health Net Medical Plan Change Request Form to the Health Net Account Management Department. Ensure that all necessary fields are properly filled before submission.
What supporting documents are required with this form?
This form must be accompanied by the Summary of Benefits and Coverage (SBC) for each individual listed. Ensure you have these documents ready before submission.
What are common mistakes to avoid when filling out the form?
Be cautious to fill in all required fields completely and accurately, especially group contact information and member details. Missing data can delay processing.
How long does it take to process the form after submission?
Processing times can vary based on workload and the specifics of your submission. Typically, you can expect a response within a few business days after submission.
Are there any fees associated with submitting the Health Net Medical Plan Change Request Form?
There are generally no fees for submitting this form itself, but check with your insurance provider for any potential fees related to plan changes.
Related Forms








Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.