Last updated on Mar 18, 2016
Get the free Provider Information Change Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Provider Info Change
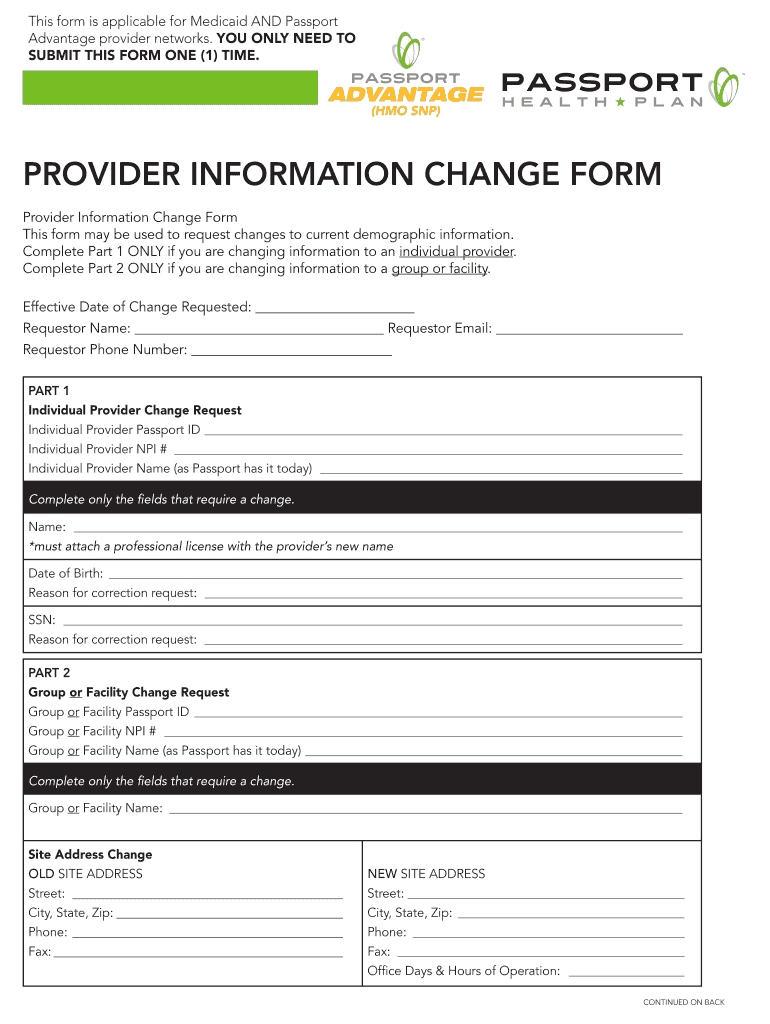
The Provider Information Change Form is a medical billing document used by healthcare providers to request changes to their demographic information for Medicaid and Passport Advantage networks.
pdfFiller scores top ratings on review platforms
Who needs Provider Info Change?
Explore how professionals across industries use pdfFiller.

Provider Info Change is needed by:
-
Healthcare providers updating their information
-
Medicaid administrators processing demographic changes
-
Office staff managing provider networks
-
Insurance companies requiring updated provider details
-
Group or facility administrators overseeing provider data
Comprehensive Guide to Provider Info Change
What is the Provider Information Change Form?
The Provider Information Change Form serves a critical purpose in the healthcare sector by allowing Medicaid and Passport Advantage providers to update their demographic information. This form is essential for maintaining accurate records within provider networks and ensures compliance with regulatory standards. By submitting this form, healthcare providers can effectively communicate any changes that affect their status, ultimately supporting better healthcare delivery.
Why is the Provider Information Change Form Important?
Keeping provider information current is necessary for compliance with healthcare regulations and for ensuring effective care delivery. Accurate records within provider networks are vital, as they facilitate communication between healthcare entities and improve overall patient management. Timely submissions of the provider information change form can prevent potential disruptions in service and enhance operational efficiency.
Who Needs to Complete the Provider Information Change Form?
The provider information change form is intended for both individual healthcare providers and group facilities. Scenarios that may prompt the need for completion include changes to address, contact information, or specific provider details. Understanding who needs to fill out this Medicaid enrollment form can help ensure that healthcare networks remain updated and functional.
How to Fill Out the Provider Information Change Form Online
Filling out the Provider Information Change Form online is straightforward. Follow these steps for successful completion:
-
Access the form on the pdfFiller platform.
-
Carefully enter your provider ID and personal details in the required fields.
-
Review key sections, particularly ensuring the accuracy of contact information.
-
Finalize your changes, and make sure all necessary fields are completed.
Utilizing pdfFiller not only simplifies this process but also enhances the accuracy of the information submitted.
Common Errors to Avoid When Submitting the Provider Information Change Form
Several common mistakes can hinder the submission process. To avoid issues when filling out the form, consider the following:
-
Double-check that all relevant fields are completed.
-
Ensure that your provider ID is accurate and up-to-date.
-
Confirm that your contact information is correctly entered.
Having a validation checklist can also streamline your submission, ensuring that all entries are accurate before sending.
Submission Methods for the Provider Information Change Form
There are multiple methods for submitting the provider information change form, including:
-
Email: Send your completed form to the designated healthcare agency.
-
Fax: Use a secure fax line to transmit your details.
-
Mail: Post the form to the appropriate office address.
Regardless of the method chosen, it is advisable to seek confirmation of receipt to ensure your submission is processed without delay.
What Happens After You Submit the Provider Information Change Form?
Once the provider information change form is submitted, you can expect specific timelines and processes. Tracking the status of your request is essential; typically, a response will be provided within a specified timeframe. If follow-up is necessary, be prepared to provide any additional required information.
Security and Compliance When Using the Provider Information Change Form
pdfFiller prioritizes user data security and compliance with regulations during the form-filling process. Adhering to HIPAA and GDPR guidelines ensures that sensitive healthcare information remains protected while users complete their forms. This commitment to security offers peace of mind for all users navigating this important documentation.
Using pdfFiller to Streamline Your Provider Information Change Request
Leveraging pdfFiller’s tools can significantly enhance your experience when handling the provider information change form. Users can edit, fill, eSign, and submit documents seamlessly through the platform. This not only simplifies the required processes but also ensures that all healthcare documentation is managed securely and efficiently.
Resources and Support for Completing the Provider Information Change Form
For additional assistance while filling out the provider information change form, resources and support options are readily available. Users can access help documents related to the form’s requirements and reach out to customer service for personalized support. This ensures that all queries are addressed promptly, facilitating a smoother form completion process.
How to fill out the Provider Info Change
-
1.Access the Provider Information Change Form on pdfFiller by searching for the form name or navigating through the healthcare forms category.
-
2.Once the form is open, familiarize yourself with the provided sections, including individual and group changes.
-
3.Gather essential information such as your provider ID, current name, address, and contact information before you start filling out the form.
-
4.Begin completing the fields by clicking into each section. Use pdfFiller's tools, such as text boxes or checkboxes, as indicated in the form.
-
5.Fill in any blank fields carefully. Make sure to include all necessary details to avoid delays in processing your request.
-
6.Utilize the tips and instructions provided within the form for any specific requirements or additional information needed.
-
7.After completing the form, review all entered data for accuracy and completeness to ensure all required fields are included.
-
8.Finalize your document by saving your changes on pdfFiller. You can also choose to download the completed form for your records.
-
9.Submit the completed form directly through pdfFiller via email, or choose to print and fax or mail it to the appropriate address as instructed.

Who needs to fill out the Provider Information Change Form?
Healthcare providers who need to update their demographic information, including names, addresses, or contact details for Medicaid or Passport Advantage networks, should fill out this form.
What are the submission methods for this form?
The completed Provider Information Change Form can be submitted via email, fax, or mailed to the specified address. Be sure to follow the instructions provided to ensure successful submission.
Are there any deadlines for submitting this form?
While specific deadlines can vary, it is generally advisable to submit changes as soon as they occur to avoid disruptions in provider network status. Check with Medicaid for exact timelines.
What supporting documents are required with this form?
Typically, no additional documents are required unless stated otherwise in the form instructions. However, having identification and verification of the changes may be useful.
What common mistakes should I avoid while filling out this form?
Ensure all required fields are completed accurately, check for typos in IDs and contact information, and follow the instructions precisely to avoid processing delays.
How long does it take to process the Provider Information Change Form?
Processing times can vary. While some changes may be updated quickly, others could take several weeks. It’s best to inquire with Medicaid for their specific timelines.
Can I make changes to this form after submitting it?
Once the Provider Information Change Form has been submitted, it generally cannot be altered. If changes are necessary, you may have to submit a new form.
Related Forms








Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.