Last updated on Mar 18, 2016
Get the free My Health/My Choices Incentive Program Contact Information Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Health Incentive Form
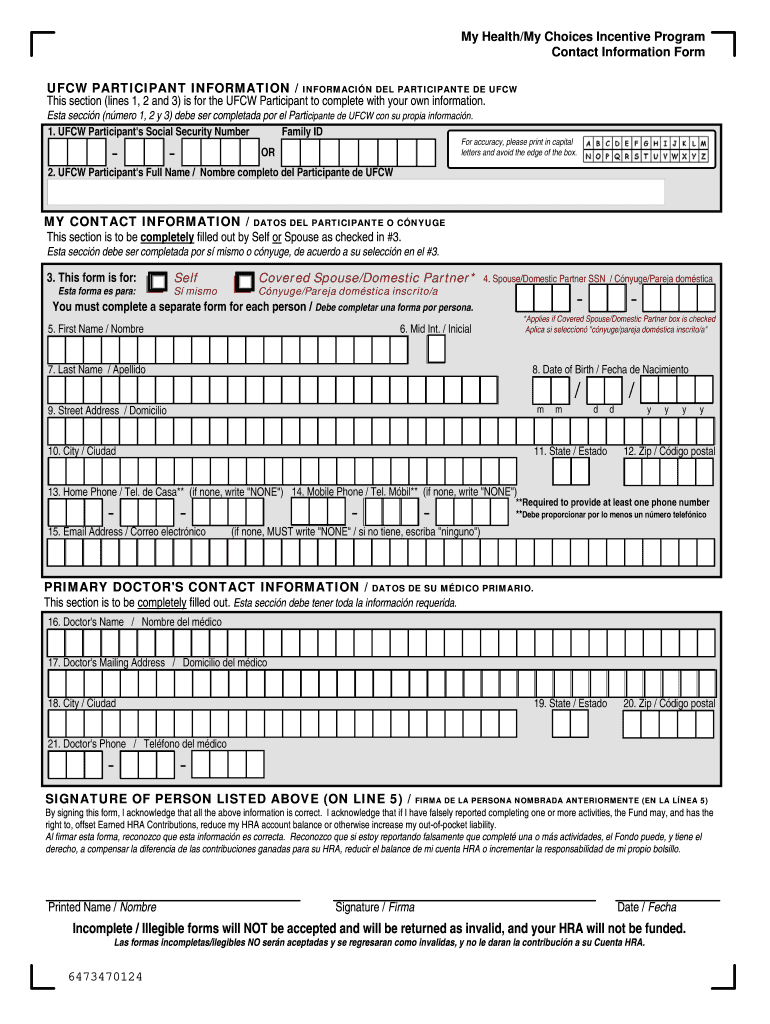
The My Health/My Choices Incentive Program Contact Information Form is a healthcare document used by UFCW participants to update their contact information for receiving Earned Health Reimbursement Account contributions.
pdfFiller scores top ratings on review platforms
Who needs Health Incentive Form?
Explore how professionals across industries use pdfFiller.

Health Incentive Form is needed by:
-
UFCW Participants of the Indemnity PPO Medical Plan
-
Spouses or domestic partners of UFCW participants
-
Individuals aimed at receiving HRA contributions
-
Beneficiaries requiring updated contact info
-
California residents participating in health incentive programs
Comprehensive Guide to Health Incentive Form
What is the My Health/My Choices Incentive Program Contact Information Form?
The My Health/My Choices Incentive Program Contact Information Form is crucial for Indemnity PPO Medical Plan Participants and their covered spouses or domestic partners. This health incentive form allows participants to provide accurate and up-to-date contact information, which is essential for timely communication regarding their health benefits. Using the contact information form ensures that all participants receive important updates and notices related to the program.
Purpose and Benefits of the My Health/My Choices Incentive Program Contact Information Form
The main purpose of this form is to facilitate the Earned Health Reimbursement Account (HRA) Contribution, which enhances participant engagement with their healthcare plans. By completing the medical plan form, participants can access a variety of resources that support their health needs. Updating contact information also helps ensure timely communication, so participants don’t miss valuable updates or health resources.
Eligibility Criteria for the My Health/My Choices Incentive Program Contact Information Form
To qualify as a UFCW participant and utilize the California health form, individuals must meet specific criteria. This includes being an enrolled participant in the Indemnity PPO Medical Plan and having eligible dependents, such as partners or spouses. It's important for participants to check their state-specific eligibility requirements to fully benefit from this health reimbursement account.
How to Fill Out the My Health/My Choices Incentive Program Contact Information Form Online
Filling out the contact information form online is straightforward. Participants should follow these steps:
-
Open the form in pdfFiller.
-
Enter your Social Security Number and Full Name in the designated fields.
-
Complete any additional required fields and ensure all entries are filled.
-
Review your information carefully before submission.
-
Sign the form electronically using the e-signature feature.
pdfFiller makes it easy to complete the participant information form efficiently.
Common Errors and How to Avoid Them While Completing the Form
Completing the health incentive form can sometimes lead to common mistakes. Participants should be aware of typical errors, such as:
-
Omitting required fields
-
Inputting incorrect information
-
Failing to sign the form
To avoid these pitfalls, it is crucial to double-check all entries before submission and ensure that each field is completed accurately. Thorough validation and regular reviews can significantly reduce submission errors.
How to Submit the My Health/My Choices Incentive Program Contact Information Form
Participants can submit the medical plan form through various methods. They can either mail it directly to the Fund Office or use digital submission options where available. Adhering to submission deadlines, such as the May 31, 2015 date, is essential for maintaining eligibility. After filing, participants should keep track of their submission status to confirm receipt.
Consequences of Not Filing or Late Filing the My Health/My Choices Incentive Program Contact Information Form
Not filing or submitting the form late can have significant repercussions on HRA contributions. Participants may miss out on benefits due to compliance timelines that are strictly enforced. Understanding these potential negative impacts is crucial, as real-life examples illustrate how delays can affect access to funds that support health-related expenses.
The Role of pdfFiller in Completing the My Health/My Choices Incentive Program Contact Information Form
pdfFiller plays a vital role in simplifying the form completion process. Its capabilities include efficient editing and management of forms while ensuring the security of personal data with features like HIPAA compliance. By utilizing pdfFiller, participants can enjoy a streamlined experience when filling out the medical contact form, benefiting from easy eSigning and secure document handling.
Sample or Example of a Completed My Health/My Choices Incentive Program Contact Information Form
Having a template or example of a filled-out form can be immensely helpful. This section highlights how to complete each part of the participant information form accurately. Users should pay attention to common pitfalls identified in the sample to ensure their submissions are complete and correct.
Getting Started with pdfFiller to Fill Out Your Form Today
Starting with pdfFiller is quick and user-friendly. Users are encouraged to explore the platform's features for filling out the contact information form with ease. The benefits of completing the form online, supported by pdfFiller’s tools, make the experience straightforward and efficient, ensuring users can navigate the process without hassle.
How to fill out the Health Incentive Form
-
1.Access the My Health/My Choices Incentive Program Contact Information Form on pdfFiller by searching for the form in the document library.
-
2.Once the form is open, familiarize yourself with the layout and navigation features provided by pdfFiller.
-
3.Before filling out the form, gather essential information such as your Social Security Number, full name, and your primary doctor's contact details.
-
4.Start by filling in the blank fields such as the UFCW Participant's Full Name and Social Security Number. Use the fillable fields in the pdfFiller interface to enter this information directly.
-
5.Navigate to checkboxes and ensure you make selections where necessary, especially those relevant to your personal circumstances.
-
6.Review all completed fields for accuracy. It's crucial to double-check details like your contact information and that of your primary doctor.
-
7.Finalize the form by signing electronically using pdfFiller's signature feature, ensuring that your signature is clear and meets the document's requirements.
-
8.Once complete, save your work to avoid losing any information. Use the 'Save' button to keep a copy of the filled form.
-
9.Download the filled document or submit it directly through pdfFiller. Follow the on-screen prompts to share it with the Fund Office.

Who is eligible to fill out this form?
Eligibility to fill out the My Health/My Choices Incentive Program Contact Information Form includes UFCW participants of the Indemnity PPO Medical Plan and their spouses or domestic partners who are covered under the plan.
What is the deadline for submitting this form?
The completed form must be submitted to the Fund Office by May 31, 2015, to qualify for the Earned Health Reimbursement Account contribution for the program year.
How do I submit the form once completed?
You can submit the completed form directly through pdfFiller by following the submission prompts after you finalize your entries. Alternatively, you can download it and send it to the Fund Office via mail.
What should I do if I need help completing the form?
If you encounter difficulties while completing the form, refer to the help section on pdfFiller or seek assistance from a knowledgeable friend or family member familiar with health forms.
Are there any common mistakes I should avoid?
Common mistakes include leaving blank fields, miswriting your Social Security Number, or forgetting to sign the form. Always double-check your entries before submission.
How long does it take to process the form after submission?
Processing times may vary, but typically allow a few weeks for the Fund Office to process your submitted information and apply it to your Health Reimbursement Account.
Do I need to provide any supporting documents?
No additional supporting documents are required with the My Health/My Choices Incentive Program Contact Information Form itself, but you may need to have your health plan or Social Security documents available for personal reference.
Related Forms






Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.