Last updated on Mar 18, 2016
Get the free Prescription Reimbursement Claim Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Prescription Claim Form
The Prescription Reimbursement Claim Form is a healthcare document used by patients to request reimbursement for prescription medication costs from their insurance provider.
pdfFiller scores top ratings on review platforms
Who needs Prescription Claim Form?
Explore how professionals across industries use pdfFiller.

Prescription Claim Form is needed by:
-
Patients who purchase prescription medications
-
Healthcare providers who assist in the claims process
-
Insurance companies processing reimbursement requests
-
Pharmacies that dispense medications
-
Plan participants enrolled in health insurance plans
Comprehensive Guide to Prescription Claim Form
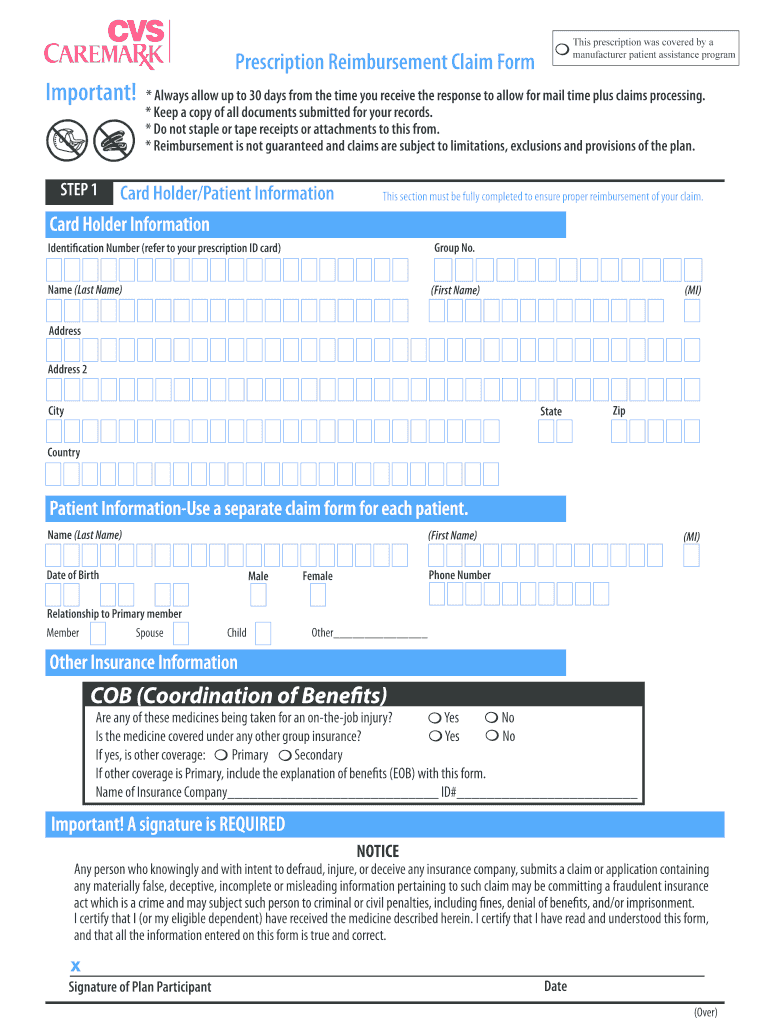
What is the Prescription Reimbursement Claim Form?
The Prescription Reimbursement Claim Form is a vital document required for patients to seek financial reimbursement from their health insurance providers for prescription medication costs. This form captures essential details, including patient information such as name, address, and date of birth, alongside pharmacy data, including the pharmacy's name and contact information. Completing this form accurately ensures a smooth claim submission process, facilitating timely reimbursement for prescription expenses.
Purpose and Benefits of the Prescription Reimbursement Claim Form
The primary purpose of the Prescription Reimbursement Claim Form is to streamline the reimbursement process for medication costs incurred by patients. By submitting this form, individuals can significantly reduce their out-of-pocket expenses, making healthcare more affordable. Additionally, this form simplifies the claim submission process, allowing users to easily manage their healthcare finances and track reimbursement requests with their insurance providers.
Who Needs to Use the Prescription Reimbursement Claim Form?
This form is essential for a variety of individuals, particularly plan participants who have incurred costs for prescription medications. It is important for eligible patients to know when to file a claim; those who have coverage that allows for reimbursements for out-of-pocket expenses will find this form necessary. Understanding the eligibility criteria helps ensure that users can efficiently process their claims and receive the financial assistance they deserve.
State-Specific Guidelines for the Prescription Reimbursement Claim Form
Regulations surrounding the Prescription Reimbursement Claim Form may differ from state to state. For instance, residents in Arizona, California, Pennsylvania, and D.C. are subject to specific rules that could affect how claims are processed. Common variations may include unique requirements for documentation and submission timelines. Patients must familiarize themselves with their state's regulations to avoid potential pitfalls that could delay their reimbursement.
Completing the Prescription Reimbursement Claim Form: A Step-by-Step Guide
Accurate completion of the Prescription Reimbursement Claim Form is crucial for successful claim submission. Follow these steps to ensure all information is correctly filled out:
-
Enter personal information, including your name and contact details.
-
Detail the prescription specifics, such as medication name and dosage.
-
Provide pharmacy information, including the pharmacy’s name and address.
-
Sign the form where indicated to authenticate your submission.
Taking these steps will enhance the likelihood of a successful claim and timely reimbursement.
Submission Process for the Prescription Reimbursement Claim Form
Once the form is completed, there are several methods for submission. Patients can opt to submit their forms online or by mail, depending on their preferences and the options provided by their insurance carriers. Important details to keep in mind include specific submission deadlines, any potential fees associated with filing, and the documentation that must accompany the form to support the reimbursement request.
Common Mistakes to Avoid with the Prescription Reimbursement Claim Form
When completing the Prescription Reimbursement Claim Form, users often make several common mistakes that can delay processing. Here’s a checklist to ensure accuracy before submitting:
-
Verify that all mandatory fields are filled in completely.
-
Ensure patient and pharmacy information is correctly spelled.
-
Double-check that the correct prescription details are included.
-
Adhere to submission guidelines relevant to your state.
A thorough review of these items can help prevent unnecessary delays in reimbursement.
What Happens After Submission?
After submitting the Prescription Reimbursement Claim Form, users can expect a processing timeline to commence. Insurance providers typically send a confirmation of receipt, allowing patients to track their claim status. It is important for users to be aware of the review process and any potential follow-up actions that may be necessary. Knowing what to expect can alleviate anxiety during the reimbursement journey.
Utilizing pdfFiller for Your Prescription Reimbursement Claim Form Needs
pdfFiller offers a user-friendly platform that simplifies the completion of the Prescription Reimbursement Claim Form. Users can easily fill out, edit, and sign the form, ensuring that all necessary information is presented accurately. Additionally, pdfFiller adheres to stringent security measures, including 256-bit encryption, reinforcing user confidence in protecting sensitive data while managing their healthcare forms.
Ensure Smooth Reimbursement: Take Action Now!
Utilize the services provided by pdfFiller to handle prescription reimbursement claims efficiently. By creating an account, users can take advantage of the platform’s robust capabilities to manage their healthcare forms with ease and security. Embrace the convenience that pdfFiller offers in streamlining the claims process, ultimately improving your experience with medication reimbursement.
How to fill out the Prescription Claim Form
-
1.Access the Prescription Reimbursement Claim Form on pdfFiller by searching for its official name in the template library.
-
2.Once the form opens, familiarize yourself with the layout and available fillable fields.
-
3.Gather necessary information, including your name, address, date of birth, and details about the prescription and pharmacy.
-
4.Input your personal information into the corresponding fields: enter your full name, complete address, and date of birth accurately.
-
5.Fill in the prescription details, including the medication name, prescription number, and the pharmacy's name and address.
-
6.Make sure to include your health insurance details where prompted on the form.
-
7.Once you have completed all fields, review the form for any errors or omissions, ensuring all information is accurate.
-
8.Use pdfFiller’s editing tools to make any adjustments as necessary before finalizing the document.
-
9.To finalize, click the save option to store a copy of your completed form on your device.
-
10.You can download the form or submit it directly to your insurance company through pdfFiller’s submission options to ensure a timely reimbursement process.

Who is eligible to use the Prescription Reimbursement Claim Form?
Any patient who has incurred expenses for prescription medications and has health insurance coverage that allows for reimbursement can use this form.
What supporting documents are required when submitting this form?
You will typically need to include prescription receipts and any other related documentation requested by your insurance provider along with the completed claim form.
Are there deadlines for submitting the Prescription Reimbursement Claim Form?
Yes, each insurance provider has specific deadlines for claim submissions. It’s vital to check with your provider for their specific timeframes to ensure your claim is processed successfully.
What common mistakes should I avoid when filling out this form?
Ensure all personal information is accurate and that you fill in all required fields. Double-check for errors in prescription details and ensure all documents are attached before submission.
How will my claim be processed, and how long does it take?
Claims processing times vary by insurance company. Typically, you can expect a response within a few weeks. Check with your insurer for specific processing timelines.
Can I submit the Prescription Reimbursement Claim Form online?
Yes, you can submit your completed form electronically through pdfFiller or check with your insurance provider for their specific submission methods.
What should I do if my claim is denied?
If your claim is denied, review the denial notice for specific reasons. You can often appeal the decision by providing additional documentation or correcting any issues noted by the insurer.
Related Forms


Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.