Last updated on Mar 18, 2016

Get the free Prior Authorization Questionnaire for Zorvolex
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Zorvolex Authorization
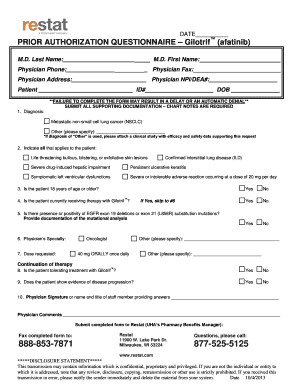
The Prior Authorization Questionnaire for Zorvolex is a healthcare form used by physicians to request authorization for prescribing Zorvolex (diclofenac) capsules.
pdfFiller scores top ratings on review platforms
Who needs Zorvolex Authorization?
Explore how professionals across industries use pdfFiller.

Zorvolex Authorization is needed by:
-
Physicians prescribing Zorvolex
-
Medical facilities needing prior authorization
-
Patients seeking prescription coverage
-
Pharmacists processing prescriptions
-
Insurance companies reviewing claims
Comprehensive Guide to Zorvolex Authorization
Understanding the Prior Authorization Questionnaire for Zorvolex
The Prior Authorization Questionnaire for Zorvolex is essential for healthcare professionals. This specific form serves the significant purpose of aiding physicians in requesting Zorvolex prescriptions efficiently. It requires detailed patient information, especially regarding their history with diclofenac, to facilitate the authorization process.
Understanding the form's structure and purpose is critical for ensuring appropriate patient care and compliance with insurance requirements.
Benefits of Using the Prior Authorization Questionnaire for Zorvolex
Utilizing the Prior Authorization Questionnaire provides numerous advantages for physicians and their patients. Primarily, it simplifies the authorization process, making it easier for healthcare providers to secure the necessary approvals quickly.
Moreover, it enhances compliance with insurance regulations, ultimately saving time for both patients and healthcare professionals, which is crucial in today's fast-paced medical environment.
Key Features of the Prior Authorization Questionnaire for Zorvolex
This form includes several important components aimed at streamlining the authorization process. Among the fillable fields are:
-
M.D. Last Name
-
Patient ID#
-
Physician Phone
-
Checkboxes for patient history responses
The necessity of the physician's signature on the document cannot be overstated, as it reinforces the legitimacy of the request and may require additional documentation as support.
Who Should Use the Prior Authorization Questionnaire for Zorvolex?
The primary users of this questionnaire are physicians who prescribe Zorvolex. However, understanding the patient demographics that may require this authorization is also essential.
Eligibility to complete the form typically applies to patients who have a documented medical need for Zorvolex and who are facing prior authorization requirements in the U.S.
Steps to Complete the Prior Authorization Questionnaire for Zorvolex
Completing the Prior Authorization Questionnaire involves a series of specific steps. Here’s a guide to fill out the form online:
-
Access the form through the appropriate healthcare provider portal.
-
Fill in all required fields, including patient and physician details.
-
Check for accuracy in responses, especially regarding patient history with diclofenac.
-
Review the form for completeness before submission.
Common errors to avoid include missing patient information or failing to sign the document, both of which could delay the authorization process.
Required Supporting Documents for Submission
Accompanying the completed Prior Authorization Questionnaire are crucial supporting documents. These include:
-
Chart notes that substantiate the medical necessity for Zorvolex.
-
Previous treatment records indicating prior diclofenac usage.
Creating a checklist before submission can help ensure all necessary documents are prepared and sent with the form.
Submission Process for the Prior Authorization Questionnaire for Zorvolex
Submitting the questionnaire can be done through multiple methods. Available submission options include:
-
Online submission via the healthcare provider's portal.
-
Mailing the completed form to the insurance provider.
Tracking options post-submission are often provided by the insurance company, and adhering to deadlines is critical to avoid complications.
Following Up on Your Submission
After submission, checking the application status is important for both patients and physicians. Users should:
-
Contact the insurance provider to inquire about the status.
-
Be aware of common rejection reasons, such as missing documentation.
If necessary, information about renewing or resubmitting the authorization can help streamline the process in case of initial rejection.
Security and Compliance When Handling Patient Information
Secure handling of sensitive patient data is paramount throughout the authorization process. pdfFiller ensures compliance with HIPAA and GDPR regulations, reinforcing the trustworthiness of their services.
Healthcare professionals must prioritize data protection to maintain patient confidentiality while managing authorization forms effectively.
Enhance Your Documentation Experience with pdfFiller
Using pdfFiller streamlines the form-filling process for healthcare professionals. The platform enhances the efficiency of filling, editing, and eSigning documents.
With secure cloud capabilities, users can easily manage medical forms in a reliable environment, promoting better patient care through efficient documentation practices.
How to fill out the Zorvolex Authorization
-
1.Begin by accessing pdfFiller and logging into your account.
-
2.Search for the 'Prior Authorization Questionnaire for Zorvolex' in the template library.
-
3.Once located, click on the form to open it in the editing interface.
-
4.Before starting, gather necessary patient information, including the patient’s ID, prior use of generic diclofenac, and prescribed dosage.
-
5.Navigate through the fillable fields, entering required information such as 'M.D. Last Name' and 'Physician Phone'.
-
6.For each question requiring a response, utilize the checkboxes for 'Yes' or 'No' as appropriate.
-
7.Double-check all entries for accuracy, ensuring no fields are left incomplete.
-
8.Review the signature line, and digitally sign the form if using pdfFiller’s e-signature feature.
-
9.Finalize your edits by reviewing the entire form for correctness and completeness.
-
10.Once reviewed, save your changes to the pdfFiller account or download it directly to your device.
-
11.If applicable, use pdfFiller's submission features to send the completed form to the relevant insurance provider or medical office.

Who is eligible to use the Prior Authorization Questionnaire for Zorvolex?
Physicians looking to prescribe Zorvolex and seek insurance coverage must utilize this form. It is specifically designed for medical professionals involved in patient treatment.
What supporting documents are required with the form?
Along with the Prior Authorization Questionnaire, physicians should submit relevant supporting documentation such as patients' chart notes detailing treatment history and prescribed dosage.
Are there deadlines for submitting this form?
Although specific deadlines can vary by insurance provider, it's recommended to submit the form promptly after determining the need for authorization to avoid treatment delays.
How can I submit the completed form?
You can submit the completed form through pdfFiller directly if you choose the submission feature or print it and send it through traditional mail to the insurance provider.
What common mistakes should I avoid when filling out the form?
Common mistakes include leaving fields blank, failing to provide accurate patient information, and not including necessary supporting documents, all of which can delay authorization.
How long does it take for the authorization to be processed?
Processing times vary based on the insurance provider, but it generally takes a few days to a couple of weeks. Check with your provider for specific timelines.
Can a patient fill out this form on their own?
While a patient can assist in providing information, the form must be completed and signed by a physician. It is a medical authorization document, typically requiring a professional’s input.
Related Forms

Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.