Last updated on Mar 19, 2016
Get the free CMS-1500 Dental Claim Adjustment Request
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Dental Claim Adjustment
The CMS-1500 Dental Claim Adjustment Request is a medical billing form used by healthcare providers to request adjustments to previously paid dental claims in Oklahoma.
pdfFiller scores top ratings on review platforms
Who needs Dental Claim Adjustment?
Explore how professionals across industries use pdfFiller.

Dental Claim Adjustment is needed by:
-
Dental providers seeking to adjust claim payments
-
Billing specialists managing dental claims
-
Healthcare administrators overseeing patient billing processes
-
Insurance companies assessing claim adjustments
-
Medicare and Medicaid crossover participants
-
Dental clinics and practices addressing billing discrepancies
Comprehensive Guide to Dental Claim Adjustment
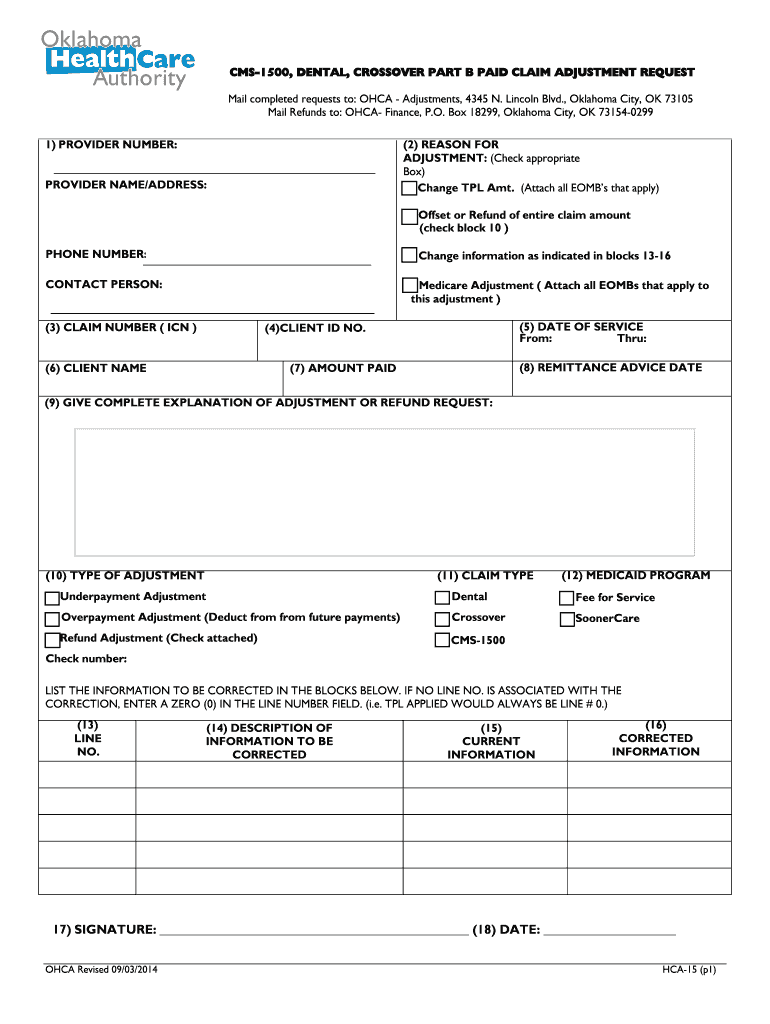
What is the CMS-1500 Dental Claim Adjustment Request?
The CMS-1500 Dental Claim Adjustment Request form is a crucial document used by healthcare providers in Oklahoma to request adjustments to previously submitted dental claims. This form plays an essential role in the healthcare billing process, ensuring that providers can correct and clarify claims to receive proper reimbursements. The form is utilized by various professionals, including dentists and dental office administrators, in scenarios where there have been errors in payment or discrepancies that need addressing.
Understanding the significance of the CMS-1500 Dental Claim Adjustment Request is vital for maintaining an efficient revenue cycle within dental practices.
Purpose and Benefits of the CMS-1500 Dental Claim Adjustment Request
This form serves as a formal mechanism for healthcare providers to facilitate smoother billing processes. By submitting a dental billing adjustment request, practitioners can rectify mistakes or address any issues such as underpayment or claim denials. The main benefits of using this form include ensuring accurate reimbursements and expediting resolution of claims disputes, which ultimately enhances financial performance for dental practices.
Key Features of the CMS-1500 Dental Claim Adjustment Request
The CMS-1500 Dental Claim Adjustment Request comprises several key components, including fields that require specific details such as the provider's information and the claim number. When adjusting a claim, providers have access to checkboxes that allow them to indicate the type of adjustment needed, whether it’s for underpayment, overpayment, or refunds. A critical aspect of this process is the required provider signature, which validates the request and signifies its authenticity.
Who Needs the CMS-1500 Dental Claim Adjustment Request?
This form is primarily targeted at healthcare providers operating within Oklahoma. Eligibility for requesting adjustments generally includes dentists, dental hygienists, and other related professionals who wish to amend previously submitted claims. Commonly applicable claims for adjustment involve those that have resulted in financial discrepancies or require clarification.
When and How to File the CMS-1500 Dental Claim Adjustment Request
Filing the CMS-1500 Dental Claim Adjustment Request should be done promptly after the initial claim submission, ideally within a specific timeframe outlined by the payer. The filing process involves gathering essential information such as the initial claim number and the reasons for adjustments. Proper organization of documents and understanding of the expected timeline can significantly influence the outcome of the submission.
How to Fill Out the CMS-1500 Dental Claim Adjustment Request: A Step-by-Step Guide
To effectively complete the CMS-1500 Dental Claim Adjustment Request, follow these steps:
-
Begin by entering the provider's information in the designated fields.
-
Fill in the claim number and dates of service accurately.
-
Indicate the reason for the adjustment using the appropriate checkboxes.
-
Provide a detailed explanation of the adjustment needed in the respective section.
-
Sign and date the form to validate the request.
Common mistakes to avoid include incomplete fields and missing signatures, which can lead to delays in processing.
Review and Validation Checklist for the CMS-1500 Dental Claim Adjustment Request
Before submission, utilize this checklist to ensure all necessary information is included:
-
Verify the provider's information for accuracy.
-
Ensure the claim number is correctly stated.
-
Check that the adjustment reason is clearly indicated.
-
Confirm the form is signed and dated by the provider.
Common errors during reviews include mislabeling or omitting required fields; addressing these proactively can enhance submission success.
Submission Methods and Payment Processing for the CMS-1500 Dental Claim Adjustment Request
The CMS-1500 Dental Claim Adjustment Request can be submitted through various methods, including online via platforms like pdfFiller. When using online submission, providers should be aware of any associated fees and average processing times. Tracking the submission will allow providers to follow up on their requests, ensuring timely handling and addressing any issues if a claim is rejected.
Security and Compliance Features of Using pdfFiller
When utilizing pdfFiller to fill out the CMS-1500 Dental Claim Adjustment Request, users can rest assured about security. pdfFiller employs 256-bit encryption and adheres to compliance regulations, including HIPAA and GDPR. This commitment to security ensures that sensitive information is protected during and after the form-filling process, with secure sharing options available for added privacy.
Maximize Your Efficiency with pdfFiller for the CMS-1500 Dental Claim Adjustment Request
Using pdfFiller for your CMS-1500 Dental Claim Adjustment Request can greatly enhance your workflow. The platform provides user-friendly features such as cloud storage for easy access, editing capabilities, and options for electronic signatures. Additionally, integration within the airSlate suite presents comprehensive document management solutions that streamline your processes, making it easier to handle forms efficiently.
How to fill out the Dental Claim Adjustment
-
1.To access the CMS-1500 Dental Claim Adjustment Request form on pdfFiller, visit the pdfFiller website and use the search feature to locate the form by name.
-
2.Once you find the form, click on it to open it in the pdfFiller editor. You will see various fields pre-printed for your input.
-
3.Begin by gathering the necessary information before starting. Ensure you have your provider number, claim number, dates of service, and any documentation regarding the reason for adjustment.
-
4.Navigate through the fields using pdfFiller's interface by clicking on each blank space. Use your keyboard to enter relevant information as required.
-
5.For the 'Reason for Adjustment' section, clearly explain why you are requesting a change, whether it is due to underpayment, overpayment, or refund adjustments.
-
6.Once all necessary fields are completed, take a moment to review the entire form for accuracy. Ensure that all information is correct and coherent.
-
7.Finally, you can save the form through pdfFiller by clicking the appropriate options. Download it as a PDF or submit it directly through the platform as instructed.

Who is eligible to use the CMS-1500 Dental Claim Adjustment Request form?
This form is typically used by licensed dental providers in Oklahoma who are seeking adjustments for previously filed claims. Providers must also verify patient eligibility when submitting adjustments.
What is the deadline for submitting a claim adjustment request?
Generally, claim adjustment requests should be submitted as soon as discrepancies are noted. Check with the Oklahoma Healthcare Authority for specific deadlines related to your claims.
What are the acceptable submission methods for this form?
The CMS-1500 Dental Claim Adjustment Request can usually be submitted electronically through various billing software or directly mailed to the insurance company responsible for processing the dental claims.
What supporting documents are needed with this form?
Typically, you will need to include any documentation that supports your adjustment claim, such as explanation letters from the insurance company, copies of previous claims, and payment remittance statements.
What common mistakes should be avoided when filling out the form?
Common mistakes include missing signatures, incorrect claim numbers, and not providing sufficient details in the 'Reason for Adjustment' section. Take time to double-check all entries before submission.
How long does it take to process a claim adjustment request?
Processing times can vary depending on the insurance company, but generally, you can expect a response within 4-6 weeks after submission of the adjustment request.
Are there any fees associated with submitting the CMS-1500 adjustment request?
Typically, there are no direct fees for submitting the adjustment request itself; however, billing providers should verify any costs associated with processing claims with their specific insurance payers.
Related Forms






Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.