Last updated on Mar 19, 2016
Get the free Provider Add/Change/Term Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is Provider Form
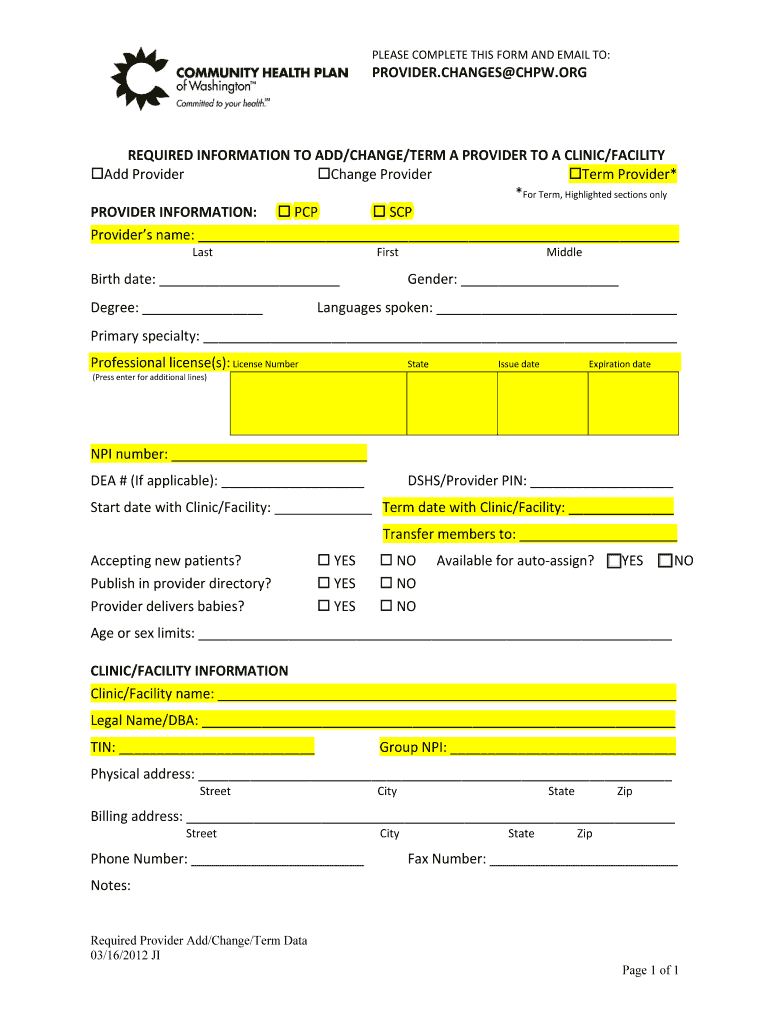
The Provider Add/Change/Term Form is a healthcare document used by administrators to add, change, or terminate a provider's association with a clinic or facility.
pdfFiller scores top ratings on review platforms
Who needs Provider Form?
Explore how professionals across industries use pdfFiller.

Provider Form is needed by:
-
Healthcare administrators managing provider records
-
Clinics updating provider information
-
Facilities terminating provider associations
-
Medical offices onboarding new providers
-
Compliance officers overseeing healthcare documentation
Comprehensive Guide to Provider Form
What is the Provider Add/Change/Term Form?
The Provider Add/Change/Term Form is essential in healthcare settings, designed to document changes in a provider's relationship with a clinic or facility. This form serves specific purposes, such as adding a new provider, updating existing provider details, or terminating a provider's association. By utilizing this healthcare provider form, facilities maintain accurate records that promote operational efficiency and compliance.
Why You Need the Provider Add/Change/Term Form
Accurate provider information is crucial within healthcare facilities. Maintaining up-to-date records minimizes risks related to compliance and enhances operational effectiveness. Failure to update provider records can lead to serious repercussions, such as regulatory penalties and disruptions in patient care. Utilizing the provider change form helps mitigate these issues by ensuring that all provider information is current and accurate.
Key Features of the Provider Add/Change/Term Form
This form contains multiple fillable fields and checkboxes, ensuring user-friendliness for those completing it. Required information includes the provider's name, birth date, and National Provider Identifier (NPI) number. With clear instructions accompanying the form, healthcare professionals can easily navigate the process of submitting the necessary information to update clinic provider information efficiently.
Who Should Use the Provider Add/Change/Term Form?
The primary audience for the Provider Add/Change/Term Form includes healthcare administrators and facility managers. These roles often require the completion of the form when adding new providers or updating existing records. Understanding who needs to use this healthcare provider form reinforces the importance of accurate documentation in maintaining facility standards.
How to Fill Out the Provider Add/Change/Term Form Online
To successfully fill out the Provider Add/Change/Term Form using pdfFiller’s platform, follow these steps:
-
Access the form through the pdfFiller interface.
-
Complete each fillable field, providing the required details accurately.
-
Review the information to ensure everything is complete and correct.
-
Save your progress as needed, then submit the form.
Providing a field-by-field explanation will help ensure that the form is filled out correctly, minimizing errors during submission.
Common Mistakes to Avoid When Completing the Provider Add/Change/Term Form
Users frequently make mistakes while filling out this form. Common issues include:
-
Leaving required fields incomplete.
-
Entering incorrect provider information.
-
Failing to double-check submitted details before sending.
To avoid these pitfalls, verify and validate all information before submission, ensuring that it aligns with existing records.
Where to Submit the Provider Add/Change/Term Form and Additional Steps
Upon completing the form, users can submit it through various methods. Both online and physical submission options are available, depending on facility preferences. After submission, confirmation of receipt will occur, and users may need to follow up if additional information is required.
Security and Compliance When Handling the Provider Add/Change/Term Form
Data protection and compliance are vital, especially concerning sensitive healthcare information. pdfFiller employs robust security measures, including 256-bit encryption, to safeguard the information within the healthcare provider form. Compliance with regulations like HIPAA and GDPR further ensures that users can submit clinic provider information with peace of mind.
Utilizing pdfFiller for the Provider Add/Change/Term Form
pdfFiller streamlines the process of completing and managing the Provider Add/Change/Term Form. Key features include eSigning capabilities, document sharing options, and accessibility from any device. These functionalities make it easier for healthcare professionals to keep their records updated efficiently and securely.
How to fill out the Provider Form
-
1.To access the Provider Add/Change/Term Form on pdfFiller, visit the pdfFiller website and search for the form using its name.
-
2.Once found, open the form in the pdfFiller editor to begin completing the fields.
-
3.Before filling out the form, gather all necessary information such as the provider's name, birth date, professional license details, and NPI number.
-
4.Navigate through the fillable fields on pdfFiller, entering information accurately as prompted, ensuring to use the appropriate format for licenses and numbers.
-
5.If applicable, check any relevant boxes that pertain to the provider's status or requirements as indicated on the form.
-
6.Use the instructions provided on the form to guide you in completing any specific sections accurately.
-
7.Once all the information is filled in, double-check all entries to ensure there are no mistakes or missing details.
-
8.Review the entire form using pdfFiller's preview feature, making any necessary adjustments before finalizing.
-
9.To save your completed form, click on the save option, allowing you to choose the desired format for download.
-
10.You can submit the form directly through pdfFiller if there is an online submission option available, or download it for mailing or emailing as preferred.

Who is eligible to use the Provider Add/Change/Term Form?
The Provider Add/Change/Term Form is intended for healthcare administrators and authorized personnel managing provider associations within clinics or facilities.
Are there deadlines for submitting this form?
While specific deadlines may vary by facility, it is advisable to submit the Provider Add/Change/Term Form as soon as a change is required to ensure compliance and accurate records.
What is the submission process for the form?
You can submit the Provider Add/Change/Term Form either online via pdfFiller or download it for postal or email submission, depending on your facility's requirements.
What supporting documents do I need to provide?
Typically, supporting documents such as the provider's professional license and NPI number should accompany the form if required by your clinic or facility’s policies.
What are common mistakes to avoid when filling out this form?
Ensure all fields are completed accurately, reviewing for spelling errors in names and numbers, and check any boxes that apply to avoid processing issues.
How long does it take to process the submitted form?
Processing times may vary; however, it's generally recommended to allow at least a couple of weeks for updates to be reflected in the system after submission.
Are there any fees associated with submitting the form?
In most cases, there are no fees for submitting the Provider Add/Change/Term Form itself, but check with your specific clinic or facility for any related processing charges.
Related Forms




Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.