Last updated on Mar 20, 2016
Get the free Dental Source Membership Change Request Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
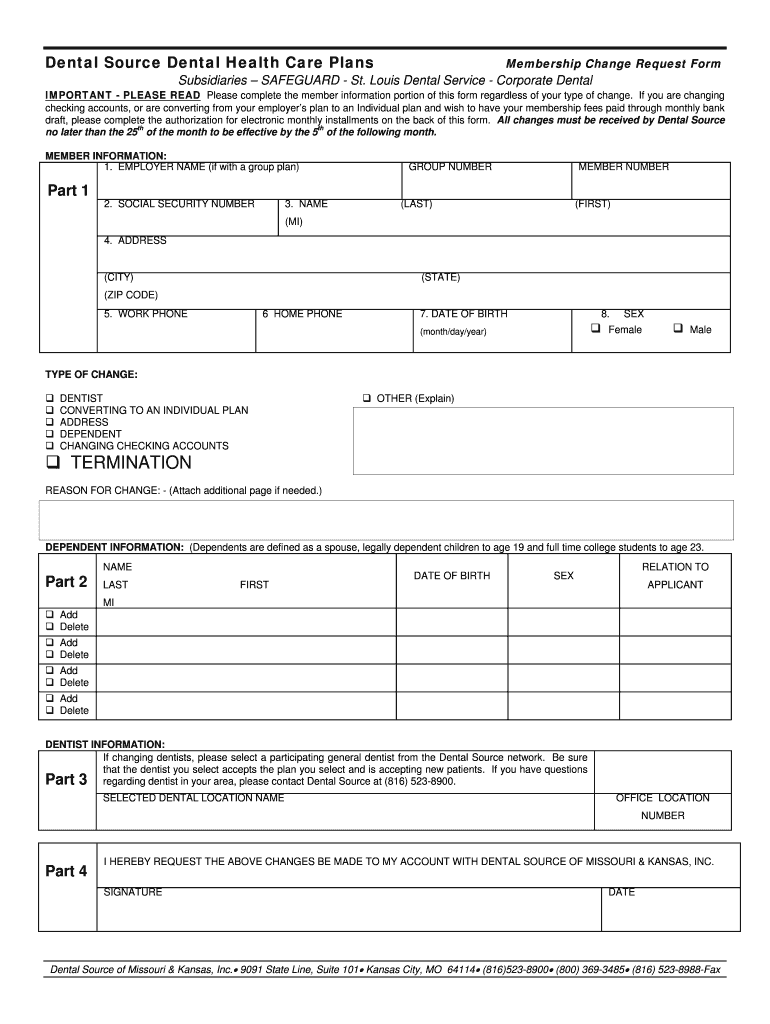
What is Dental Membership Change Form
The Dental Source Membership Change Request Form is a healthcare document used by members in Missouri and Kansas to request changes to their dental health care plans.
pdfFiller scores top ratings on review platforms
Who needs Dental Membership Change Form?
Explore how professionals across industries use pdfFiller.

Dental Membership Change Form is needed by:
-
Dental Source members seeking to update their plans
-
Individuals wanting to change dentists or addresses
-
Members looking to add or remove dependents
-
Patients opting for changes in their payment methods
-
Those converting from group plans to individual coverage
Comprehensive Guide to Dental Membership Change Form
What is the Dental Source Membership Change Request Form?
The Dental Source Membership Change Request Form is a vital tool for members of Dental Source of Missouri & Kansas, Inc. designed to request adjustments to their dental health care plans. It allows members to streamline the process of requesting changes regarding their dental plan information. This form features fillable fields, enhancing user experience and efficiency during completion.
Purpose and Benefits of the Dental Source Membership Change Request Form
The purpose of the Dental Source Membership Change Request Form is to facilitate easy access for members to update their dental plans. By utilizing this form, members can request various types of changes such as altering their preferred dentist, updating personal details, or adding and removing dependents. Timely submissions are crucial as they directly affect the effective dates of requested changes, enabling seamless transitions in coverage.
Who Needs the Dental Source Membership Change Request Form?
All members of Dental Source are eligible to submit the Dental Source Membership Change Request Form when their situation warrants a change. This includes circumstances like relocating or modifications in insurance coverage. Ensuring that all personal and dependent information remains current is essential for maintaining optimal coverage and benefit utilization.
How to Fill Out the Dental Source Membership Change Request Form Online (Step-by-Step)
Filling out the Dental Source Membership Change Request Form online is a straightforward process when following these steps:
-
Gather required personal information, including your name, address, and phone numbers.
-
Provide your employer's name and social security number.
-
Indicate the type of change you are requesting by selecting the appropriate options.
-
Complete the dependent information section as needed.
-
Enter payment details if applicable, ensuring accuracy to avoid common submission pitfalls.
Important Deadlines for Submitting the Dental Source Membership Change Request Form
Members must adhere to specific deadlines for the timely processing of their requests. The form needs to be submitted by the 25th of each month to ensure that changes take effect by the 5th of the subsequent month. Late submissions can result in delays in the implementation of adjustments, potentially affecting member benefits.
Payment Information and Options for the Dental Source Membership Change Request Form
When filling out the Dental Source Membership Change Request Form, members need to provide payment authorization details, including bank and credit card information. Security measures are implemented to protect sensitive payment data in accordance with HIPAA guidelines. Furthermore, there may be fee waivers or assistance options available for members in need.
Where to Submit the Dental Source Membership Change Request Form
Members can submit the Dental Source Membership Change Request Form through various methods. Options include:
-
Online submission via the Dental Source portal.
-
Mailing the completed form to the designated address.
-
Hand delivering the form at a local Dental Source office.
Confirming receipt is essential; members should ensure they have a tracking method or validation mechanism to verify successful submission.
What Happens After You Submit the Dental Source Membership Change Request Form
Upon submission of the form, members will receive updates regarding the status of their requested changes. Processing timelines can vary, and it’s advisable to check back if confirmation is not received within an expected timeframe. Should any issues arise, guidance is provided for status inquiries and resolution steps.
Security and Compliance for the Dental Source Membership Change Request Form
Member data protection is a top priority when using the Dental Source Membership Change Request Form. Security protocols, including encryption, are in place to safeguard personal information. Compliance with laws like HIPAA ensures that all medical and payment information is handled with utmost privacy and diligence.
Maximize Your Dental Source Membership Change Request Experience
To enhance the experience of filling out the form, members are encouraged to utilize pdfFiller. This platform simplifies the form-filling process by providing secure online functionalities, including eSigning and document management. By using pdfFiller, members can efficiently manage their healthcare documentation and streamline their requests.
How to fill out the Dental Membership Change Form
-
1.Access the Dental Source Membership Change Request Form by visiting pdfFiller's website and searching for the form name in the search bar.
-
2.Open the form by clicking on the link provided for the Dental Source Membership Change Request Form.
-
3.Familiarize yourself with the pdfFiller interface, where you can efficiently navigate the fillable fields using your mouse or keyboard.
-
4.Before you begin filling out the form, gather all necessary information including employer name, social security number, address, phone numbers, date of birth, and any details related to the changes you wish to make.
-
5.Start with the first field, 'EMPLOYER NAME', and input the required information. Continue filling in subsequent sections, ensuring to differentiate between work and home phone numbers.
-
6.If you need to indicate changes such as switching dentists or updating addresses, select the appropriate options or fill them in as directed.
-
7.Review your completion for accuracy, making sure all fields are filled out properly, as errors can delay processing.
-
8.Finalize the form by inserting your signature and the date in the designated fields.
-
9.Use pdfFiller tools to save your completed form, or download a copy for your records. To submit, follow the outlined submission instructions provided on the pdfFiller platform.

Who is eligible to use the Dental Source Membership Change Request Form?
The form is exclusively for members of Dental Source located in Missouri and Kansas who wish to make changes to their dental health care plans.
Is there a deadline for submitting the membership change request?
Yes, all requests must be submitted by the 25th of the month to be effective by the 5th of the following month, so be sure to meet this deadline.
How can I submit the completed form?
Once you have filled out the Dental Source Membership Change Request Form, submit it via the specified method on pdfFiller or according to the instructions provided by Dental Source.
What information is required when filling out the form?
Required information includes your employer name, social security number, address, phone numbers, date of birth, and detailed information about any requested changes.
What common mistakes should I avoid when completing the form?
Ensure that all fields are filled accurately, especially critical information like the social security number, and double-check spelling in case of name changes or address updates.
How long will it take for my changes to be processed?
After submission, processing times can vary, but generally, changes become effective by the 5th of the following month provided the form is submitted on time.
Do I need to notarize the Dental Source Membership Change Request Form?
No, notarization is not required for submitting the Dental Source Membership Change Request Form.
Related Forms






Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.