Last updated on Apr 6, 2026

Get the free Authorization to Use or Disclose Protected Health Information
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
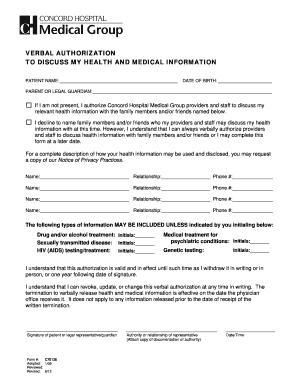
What is authorization to use or
The Authorization to Use or Disclose Protected Health Information is a healthcare form used by patients to authorize the Brattleboro Retreat to release or obtain their protected health information.
pdfFiller scores top ratings on review platforms
Who needs authorization to use or?
Explore how professionals across industries use pdfFiller.

Authorization to use or is needed by:
-
Patients seeking to share their health information.
-
Parents or guardians of minors under 14 years old.
-
Healthcare providers requesting patient information.
-
Administrative staff managing patient records.
-
Researchers needing data for healthcare improvement.
Comprehensive Guide to authorization to use or
What is the Authorization to Use or Disclose Protected Health Information?
The Authorization to Use or Disclose Protected Health Information is a critical form that enables patients to authorize the Brattleboro Retreat to release or obtain their protected health information. This document is essential for ensuring proper communication among healthcare providers and supports effective patient management.
The form requires specific details, including the patient’s name, date of birth, treatment details, and the purpose of the information release. Accurate completion of these fields is vital in the healthcare process, allowing for streamlined care and effective management of health records.
Why You Need the Authorization to Use or Disclose Protected Health Information
Utilizing the authorization form provides numerous benefits, including facilitating care by allowing healthcare providers to access relevant medical information. This improves communication among providers, which can significantly enhance patient outcomes.
Moreover, the form ensures legal protections are in place, safeguarding sensitive patient data. Timely submission of this authorization is essential for patients requiring ongoing treatment, as it helps maintain continuity of care.
Who Needs the Authorization to Use or Disclose Protected Health Information?
This authorization form should be filled out by patients, and parents or guardians for patients under 14 years old. Several situations necessitate the use of this form, such as when seeking second opinions or transferring medical records to another healthcare provider.
Eligibility criteria specify that the authorization can be signed by the patient or a parent/guardian, helping to protect the rights of minors while ensuring that necessary health information is shared in a compliant manner.
How to Fill Out the Authorization to Use or Disclose Protected Health Information Online
Accessing and completing the authorization form via pdfFiller is a straightforward process. Follow these steps for a successful submission:
-
Navigate to the pdfFiller website and create an account if you don’t already have one.
-
Locate the authorization form using the search feature on the platform.
-
Carefully fill out each required field, ensuring all information is accurate.
-
Utilize the fillable fields effectively and follow the provided instructions for each section.
This ensures that you comply with all requirements while making the process manageable and user-friendly.
Reviewing and Submitting Your Authorization to Use or Disclose Protected Health Information
Before submission, it’s critical to perform a thorough review. Consider the following checklist:
-
Confirm that all fields are completed and accurate.
-
Avoid common errors, such as missing signatures or incorrect information.
-
Decide on your submission method: online via pdfFiller or traditional paper submission.
Taking these steps can prevent delays and ensure that your authorization is processed efficiently.
What Happens After You Submit the Authorization to Use or Disclose Protected Health Information?
Upon submitting your authorization form, you can expect a detailed timeline for processing and confirmation of receipt. Understanding the potential consequences of delays or non-compliance is vital, as it may affect your ongoing treatment.
If changes or corrections are needed after submission, appropriate channels are available to address these requests quickly and effectively, ensuring that your healthcare provider has the most up-to-date information.
Security and Compliance for Your Authorization to Use or Disclose Protected Health Information
Using pdfFiller to manage your health information release form comes with peace of mind due to comprehensive security measures. The platform employs advanced encryption methods and is compliant with HIPAA and GDPR regulations, ensuring that sensitive data remains secure throughout the process.
Proper handling of protected health information is paramount, and pdfFiller guarantees confidentiality during and after form submission.
Using pdfFiller for Your Authorization to Use or Disclose Protected Health Information
pdfFiller offers a range of features that simplify the management of your authorization form. Key functionalities include editing capabilities, electronic signing, and seamless sharing options, all designed to enhance user experience.
User feedback highlights the platform's efficiency, reinforcing trust in its ability to manage important documents efficiently. Start utilizing pdfFiller’s tools to fill out your health information release form today.
How to fill out the authorization to use or
-
1.Access the Authorization to Use or Disclose Protected Health Information form on pdfFiller by searching for its title.
-
2.Once opened, familiarize yourself with the layout of the form, noting the fillable fields and checkboxes that require your attention.
-
3.Gather necessary information before starting, including your full name, date of birth, and specific details regarding the information you wish to release.
-
4.Begin filling out the form by entering your name and date of birth in the designated fields, making sure to be accurate to avoid any issues.
-
5.Specify the details of the health information to be released, including treatment dates and types of information, by following the prompts in the form.
-
6.Indicate the purpose of the request by checking the appropriate box or stating it clearly in the provided field.
-
7.Allow the patient or a parent/guardian to read all instructions and fill in relevant information before signing the document as per the guidelines provided within the form.
-
8.Review all entries carefully to ensure all sections are completed correctly, and ensure signatures are affixed where necessary, especially if a guardian is signing on behalf of a minor.
-
9.Finalize the form on pdfFiller, checking for any prompts regarding missing information that may prevent completion.
-
10.Once satisfied with the information, save the form to your files, download a copy if needed, or submit it electronically as directed by your healthcare provider.

Who is eligible to sign the Authorization form?
The Authorization to Use or Disclose Protected Health Information form must be signed by the patient or a parent/guardian if the patient is under 14 years old.
What information is required to complete the form?
You will need to provide your name, date of birth, details about the information requested for release, including treatment dates and types of information.
How long is the authorization valid?
The authorization expires six months from the date it is signed, after which a new form will be required to continue sharing information.
What should I do if I make a mistake on the form?
If you make a mistake, you should start a new form, as corrections should not be made directly on the Authorization form to maintain clarity.
How can I submit the completed form?
Completed forms can be submitted electronically through pdfFiller, printed and mailed, or taken directly to the healthcare provider's office.
Is notarization required for this form?
No, the Authorization does not require notarization, simplifying the process for patients and guardians.
What common mistakes should I avoid when filling out the form?
Common mistakes include omitting signature requirements, incorrect personal information, and failure to specify the scope of the health information requested.
Related Forms







Get the latest insights from our blog

If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.