Last updated on May 1, 2026

Get the free Patient Authorization Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
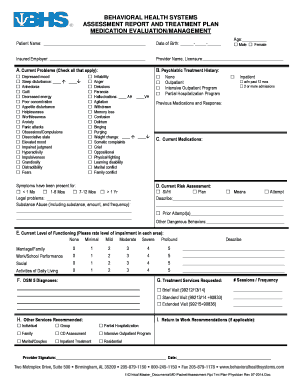
What is Patient Authorization Form
The Patient Authorization Form is a medical consent document used by patients to authorize the release of their medical information and payment to healthcare providers.
pdfFiller scores top ratings on review platforms
Who needs Patient Authorization Form?
Explore how professionals across industries use pdfFiller.

Patient Authorization Form is needed by:
-
Patients requiring medical treatment
-
Caregivers managing healthcare for patients
-
Healthcare providers needing authorization for payment
-
Insurance companies processing claims
-
Legal representatives handling medical records
Comprehensive Guide to Patient Authorization Form
What is the Patient Authorization Form?
The Patient Authorization Form is a crucial document that enables patients to authorize the release of medical information to healthcare providers. It plays an essential role in the healthcare process, particularly in Washington, D.C. Within this framework, the form ensures that patients maintain control over their medical records while allowing healthcare providers access to necessary information for treatment and billing purposes. This process is vital for both patients and providers, streamlining communication and enhancing care delivery efficiency.
Purpose and Benefits of the Patient Authorization Form
The necessity of the Patient Authorization Form stems from both legal and administrative requirements in healthcare. It serves multiple purposes, including facilitating the communication of crucial medical data between patients and providers. The benefits for patients are significant; not only does the form streamline interactions with healthcare professionals, but it also ensures that payment processes are handled efficiently. Ultimately, this form safeguards the patient's rights while ensuring that healthcare providers can deliver timely care.
Key Features of the Patient Authorization Form
This form contains several key components vital for effective use:
-
Fillable fields for vital information such as name, date of birth, and address.
-
A designated area for the patient’s signature, confirming authorization.
-
Detailed instructions for accurately completing the form.
-
Security measures to ensure sensitive information is handled appropriately.
Who Needs the Patient Authorization Form?
Various individuals may require the Patient Authorization Form in different scenarios. Patients need the form when seeking treatment at a new healthcare facility, transferring records, or when multiple authorizations are necessary for specific procedures. Understanding these situations is crucial for maintaining seamless communication during medical treatments and ensuring that patient information is shared responsibly.
How to Fill Out the Patient Authorization Form Online
Filling out the Patient Authorization Form online can be efficiently done by following these steps:
-
Navigate to the pdfFiller site and locate the Patient Authorization Form.
-
Carefully fill in the required fields such as name and date of birth.
-
Review all information for accuracy before submission.
-
Sign the form digitally to validate the authorization.
Taking the time to review the form before submission is essential to ensure all information is accurate and complete.
Submission Methods for the Patient Authorization Form
Once the Patient Authorization Form has been completed, it can be submitted through various methods:
-
Online submission through the pdfFiller platform.
-
Emailing the completed form to the designated healthcare provider.
-
Mailing a physical copy to the recipient’s office.
-
Delivering the form in person for immediate processing.
It is advisable to confirm the submission method to ensure the form reaches the intended recipient without delays.
What Happens After You Submit the Patient Authorization Form?
After submission, the Patient Authorization Form goes through a processing stage by healthcare providers. Patients can expect to receive a confirmation of receipt, informing them that their authorization is under review. Additionally, there may be follow-ups necessary to finalize and clarify any details related to the authorization.
Security and Compliance for the Patient Authorization Form
Security is paramount when handling the Patient Authorization Form. pdfFiller implements robust security measures, including encryption, to protect sensitive information. Compliance with HIPAA is crucial, ensuring that all patient data is managed in accordance with legal standards and that privacy is maintained throughout the process.
Example of a Completed Patient Authorization Form
Visual reference is available through examples of completed Patient Authorization Forms, highlighting key sections and common answers. Each segment of the filled-out form is explained for clarity, making it easier for new users to understand how to properly fill in their own forms.
Start Using pdfFiller Today for Your Patient Authorization Form Needs
Utilizing pdfFiller can significantly enhance the experience of completing the Patient Authorization Form. This platform offers an easy-to-use interface for filling out forms, along with secure tools for document management. Patients can benefit from the tool's capabilities to manage sensitive documentation without compromising security.
How to fill out the Patient Authorization Form
-
1.To start, access the Patient Authorization Form on pdfFiller by searching for it in the template library or entering the form name in the search bar.
-
2.Once you have opened the form, carefully read through the initial instructions provided to understand its requirements.
-
3.Navigate through the fillable fields, beginning with your name by clicking on the designated area and typing your personal information.
-
4.Proceed to the next fields such as Date of Birth and Address, ensuring all information is accurate and complete.
-
5.Have your insurance details ready before filling in that section, making sure to double-check the information for accuracy.
-
6.If necessary, use pdfFiller’s features to add any additional information that may be requested in the form.
-
7.Review the entire document carefully, checking for any omissions or errors that may need correcting before signing.
-
8.Utilize the signature feature on pdfFiller to add your electronic signature, confirming your authorization for the release of medical information.
-
9.After completing the form, save your work to ensure none of your entries are lost during the process.
-
10.You can then download a copy of the filled form for your records, or directly submit it through pdfFiller if applicable.

What is the purpose of the Patient Authorization Form?
The Patient Authorization Form allows patients to authorize the release of their medical information to healthcare providers and insurers, ensuring that payments can be processed efficiently.
Who needs to fill out this form?
This form is necessary for patients seeking healthcare services, caregivers managing patient treatment, healthcare providers requiring authorization, and insurance companies needing information for claims.
Are there any documents I need to attach?
Typically, you may need to provide your insurance information and identification details. Ensure you have all relevant papers at hand when filling out the form.
How do I submit the Patient Authorization Form?
You can submit the completed Patient Authorization Form through pdfFiller by using the submission features available, or you can download and send it via email or postal service to your healthcare provider.
What common mistakes should I avoid when filling out this form?
Common mistakes include missing fields, incorrect insurance information, and failing to sign the form. Be sure to review the entire document before submission to avoid these errors.
Is notarization required for this form?
No, notarization is not required for the Patient Authorization Form. You only need to provide your signature to authorize the release of your medical information.
How long does it typically take to process the authorization?
Processing times can vary but are generally quick. If submitted electronically via pdfFiller, the authorization is usually processed faster compared to physical forms.
Related Forms







If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.