Last updated on Mar 20, 2016
Get the free Physician Orders for Life-Sustaining Treatment (POLST) Florida
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
What is POLST Florida
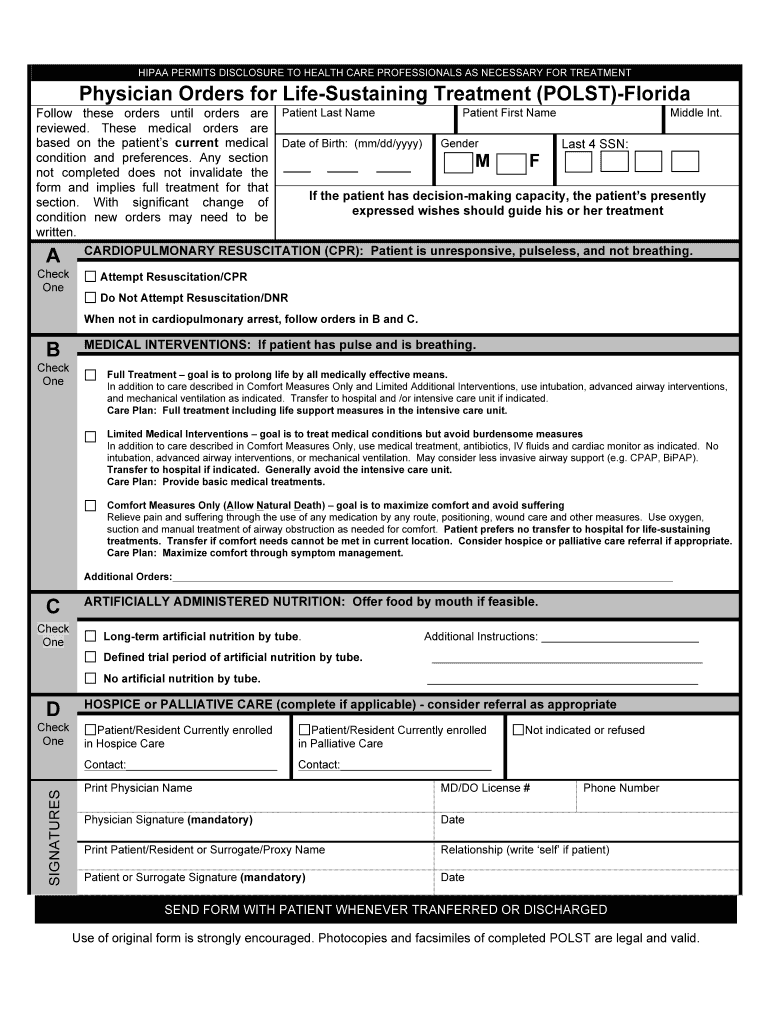
The Physician Orders for Life-Sustaining Treatment (POLST) form is a medical document used by healthcare professionals in Florida to document a patient's treatment preferences in critical care situations.
pdfFiller scores top ratings on review platforms
Who needs POLST Florida?
Explore how professionals across industries use pdfFiller.

POLST Florida is needed by:
-
Physicians managing end-of-life care
-
Patients seeking to outline their medical treatment preferences
-
Surrogates making health decisions for others
-
Healthcare facilities and providers
-
Palliative care teams
-
Hospitals and nursing homes
Comprehensive Guide to POLST Florida
What is the Physician Orders for Life-Sustaining Treatment (POLST) Florida?
The Physician Orders for Life-Sustaining Treatment (POLST) form in Florida is a crucial document designed to document patient preferences regarding medical treatment. It plays a significant role in ensuring that healthcare decisions align with individual wishes, especially in critical situations. The POLST form is essential for guiding healthcare professionals in treating patients according to their documented preferences.
This form must be signed by a healthcare professional, making it a legally binding document. By accurately reflecting the patient's desires, the POLST form helps minimize uncertainty during medical crises and supports personalized care.
Purpose and Benefits of the POLST in Florida
The POLST form is essential for both patients and healthcare providers in Florida. It ensures that patients' treatment preferences are respected, providing peace of mind during difficult times. By communicating these preferences clearly, the POLST becomes a guiding tool that can significantly impact care delivery.
-
Patients can ensure their choices regarding life-sustaining treatment are upheld.
-
Healthcare providers benefit from having clear directives that facilitate informed decision-making during emergencies.
-
Clarifying treatment options helps alleviate caregiver stress and confusion.
Who Needs the Physician Orders for Life-Sustaining Treatment (POLST) Florida?
The POLST form is primarily intended for certain patient demographics who may require clear medical directives. This includes elderly patients, individuals with severe illnesses, or anyone who wishes to specify their treatment preferences explicitly.
Surrogates, family members, and caregivers play essential roles in the process, ensuring that the patient’s wishes are clearly communicated and documented. Additionally, healthcare providers across various specialties should be familiar with the policies governing the POLST form to utilize it effectively.
How to Fill Out the POLST Form in Florida Online
Filling out the POLST form online can be simplified with a structured approach. Here are the critical fields to complete:
-
Enter the patient's last name and first name.
-
Fill in the date of birth and gender.
-
Provide the last four digits of the patient's Social Security Number.
-
Select preferences for medical interventions using fillable fields and checkboxes.
-
Ensure completion with correct signatures from both the physician and patient or surrogate.
Paying attention to detail is crucial, as any mistakes can invalidate the form.
Common Errors and How to Avoid Them
Filling out the POLST form can present challenges, leading to common errors that need to be addressed. Frequent mistakes include missing signatures, incomplete fields, and unclear handwriting that can hinder legibility.
-
Always double-check for any missing information before submission.
-
Ensure that all required signatures are present and clear.
-
Use legible handwriting or, preferably, fill out the form digitally to enhance clarity.
Digital Signature vs. Wet Signature Requirements for POLST in Florida
When completing the POLST form in Florida, understanding the signature requirements is vital. Digital signatures are accepted, providing a convenient alternative to traditional wet signatures.
This flexibility supports the needs of patients and healthcare providers by enabling quicker processing of forms. However, users should consider the context of their usage and select the signing method that best suits their requirements.
Where to Submit the POLST Form and What Happens Next
After completing the POLST form, submission options vary. It can often be submitted directly to healthcare providers or facility operations to ensure that medical teams have access to the patient's wishes.
The expected timeline for processing may vary, but tracking submission status is essential for ensuring peace of mind. Knowing where and when the form is processed allows for better planning and communication with healthcare providers.
Security and Compliance for the POLST Form
Handling the POLST form raises important privacy and security concerns. pdfFiller uses robust security measures, including 256-bit encryption and compliance with HIPAA regulations, to protect sensitive medical information.
Users can complete their POLST forms with confidence, knowing that their data is secure on digital platforms designed for safe document handling.
Experience Simplified Form Handling with pdfFiller
pdfFiller offers a user-friendly platform for managing the POLST form. With its tools for creating, editing, and eSigning forms, users can easily navigate the requirements associated with their medical directives.
-
The cloud-based accessibility allows for form management from any device without downloads.
-
Collaborative features make it easier to share and review forms with authorized parties.
Starting your POLST form with pdfFiller enhances the experience by streamlining the process, saving time, and ensuring compliance with best practices in document management.
How to fill out the POLST Florida
-
1.To access the POLST form on pdfFiller, visit the pdfFiller website and use the search bar to find the 'Physician Orders for Life-Sustaining Treatment (POLST) Florida' form.
-
2.Once located, click on the form to open it in the pdfFiller editor, which allows for easy navigation and editing.
-
3.Before filling out the form, gather essential information such as the patient's full name, date of birth, gender, and the last four digits of their Social Security Number.
-
4.In the editor, start by entering the patient's last name in the designated field, followed by their first name, and then fill in the date of birth.
-
5.Next, select the patient's gender using the provided options.
-
6.Continue by filling in the last four digits of the Social Security Number to help identify the patient.
-
7.Carefully review the medical intervention options within the form. Use the checkboxes to indicate the patient's preferences clearly.
-
8.Ensure you understand each option available for resuscitation, medical treatments, and nutrition before making selections.
-
9.Once all fields have been completed accurately, double-check the form for any errors or omissions.
-
10.To finalize the form, ensure that there are signature lines for both the physician and patient or surrogate.
-
11.After reviewing, click 'Save' to keep your completed form. You may also download it directly to your device or submit it according to your facility's protocol.

Who is eligible to complete the POLST form?
The POLST form should be completed by a licensed healthcare professional, ideally a physician, when the patient or surrogate is present to provide informed preferences about medical treatment.
Is there a deadline for submitting the POLST form?
There are no specific deadlines for completing the POLST form. However, it is crucial to have it completed and available at the time of medical emergencies to guide treatment decisions.
How do I submit the completed POLST form?
Typically, the completed POLST form should be submitted to the patient's healthcare provider, stored in their medical record, and copies should also be kept by the patient or surrogate for reference.
What supporting documents do I need to provide with the POLST form?
No additional supporting documents are typically required when completing the POLST form itself, but it may be helpful to have an advanced directive or living will for additional context.
What common mistakes should I avoid when filling out the POLST form?
Common mistakes include failing to sign the document, not properly identifying the patient, and leaving important sections blank that could affect treatment decisions.
How long does it take to process the POLST form?
Since the POLST form is a direct instruction document rather than a submission form to a governing body, there is no processing time. Its validity begins once it is signed by the physician and patient or surrogate.
Can modifications be made to the POLST form after it's completed?
Yes, modifications can be made to the POLST form at any time. However, any changes must be documented, and the updated form should be signed by the physician and patient or surrogate to ensure its validity.
Related Forms

Related Catalogs
Get the latest insights from our blog



If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.