Last updated on Mar 23, 2016
Get the free Hospital Cash Claim Form
We are not affiliated with any brand or entity on this form

Fill out
Complete the form online in a simple drag-and-drop editor.

eSign
Add your legally binding signature or send the form for signing.

Share
Share the form via a link, letting anyone fill it out from any device.

Export
Download, print, email, or move the form to your cloud storage.
Why pdfFiller is the best tool for your documents and forms
End-to-end document management
From editing and signing to collaboration and tracking, pdfFiller has everything you need to get your documents done quickly and efficiently.
Accessible from anywhere
pdfFiller is fully cloud-based. This means you can edit, sign, and share documents from anywhere using your computer, smartphone, or tablet.
Secure and compliant
pdfFiller lets you securely manage documents following global laws like ESIGN, CCPA, and GDPR. It's also HIPAA and SOC 2 compliant.
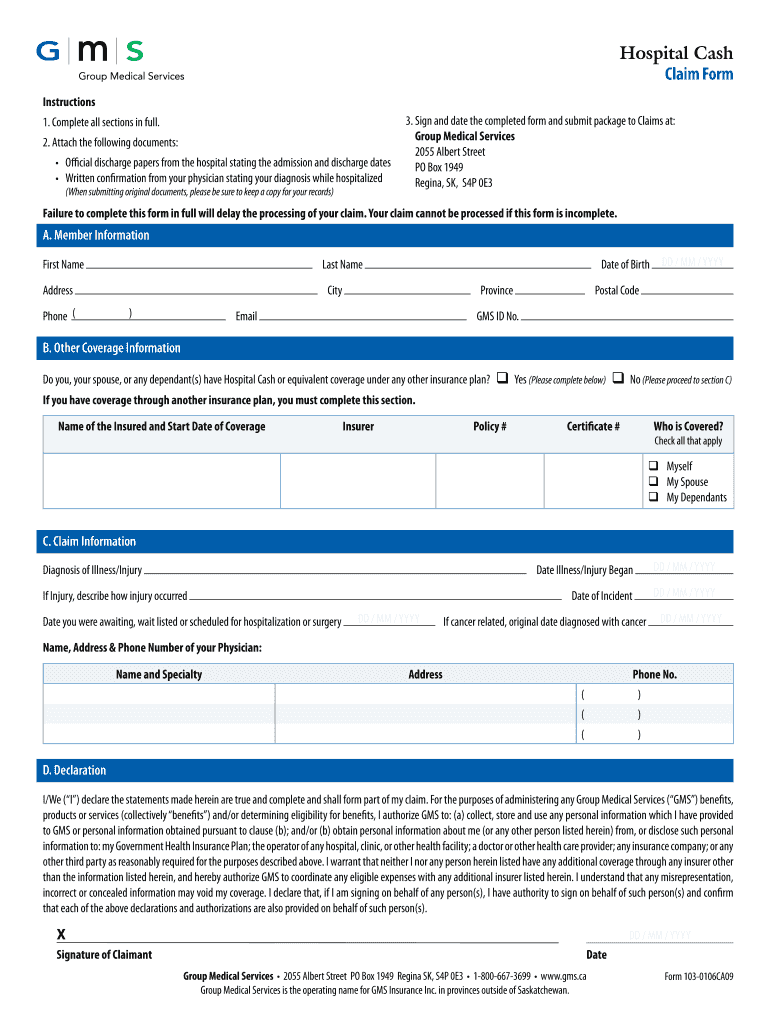
What is Hospital Claim Form
The Hospital Cash Claim Form is a health insurance claim document used by individuals to submit claims for hospital cash benefits under a group medical services insurance plan.
pdfFiller scores top ratings on review platforms
Who needs Hospital Claim Form?
Explore how professionals across industries use pdfFiller.

Hospital Claim Form is needed by:
-
Individuals seeking hospital cash benefits
-
Patients under a group medical services insurance plan
-
Healthcare providers verifying patient claims
-
Insurance agents assisting with claims
-
Family members filing on behalf of claimants
Comprehensive Guide to Hospital Claim Form
What is the Hospital Cash Claim Form?
The Hospital Cash Claim Form is designed to facilitate the submission of claims for hospital cash benefits under the Group Medical Services (GMS) insurance plan in Saskatchewan. This healthcare form plays a critical role in ensuring that claimants receive financial support for expenses related to their hospital stays. By accurately filling out this medical claim form, individuals can effectively communicate their eligibility and the details of their care to their insurance provider.
Eligibility Criteria for the Hospital Cash Claim Form
Individuals eligible to use the Hospital Cash Claim Form include those covered under specific group medical services plans. Generally, this includes residents of Saskatchewan who are enrolled in GMS insurance. Age restrictions may apply in certain cases, emphasizing the need for beneficiaries to verify their qualification based on their specific circumstances and plan guidelines.
Key Features of the Hospital Cash Claim Form
Key aspects of the Hospital Cash Claim Form include various fillable sections and required fields that guide users in completing their claims accurately. Users will find checkboxes for indicating consent and instructions to ensure clarity while filling out personal information, details about the medical situation, and the corresponding financial claims. Each section is crafted to enhance usability and precision in submissions.
When and How to File the Hospital Cash Claim Form
Claimants should be aware of the timelines for filing their claims to ensure timely processing. The submission process typically involves the following steps:
-
Complete the Hospital Cash Claim Form with accurate information.
-
Attach all required supporting documents.
-
Submit the form through your chosen method.
It’s essential to check for any deadlines associated with your specific insurance plan to avoid delays in receiving benefits.
Required Documents and Supporting Materials
To ensure your claim is processed smoothly, include the following supporting documents:
-
Discharge papers from the hospital.
-
Physician confirmation letters supporting the claim.
-
Any additional documentation that outlines the nature of the illness or injury.
Understanding the importance of each document can streamline the claim process and prevent unnecessary delays.
How to Fill Out the Hospital Cash Claim Form Online
Filling out the Hospital Cash Claim Form online requires attention to detail. Here’s a field-by-field guide:
-
Enter your personal information accurately.
-
Provide specific details regarding your hospital stay, including dates and services received.
-
Double-check all required fields to minimize errors.
Common mistakes include leaving sections blank or incorrect information, so it’s critical to review the form thoroughly before submission.
Common Errors and How to Avoid Them
Claimants often make several frequent mistakes when submitting the Hospital Cash Claim Form. Here are tips to avoid errors:
-
Ensure all fields are filled correctly, especially those marked as required.
-
Review the form for any missing signatures or dates.
-
Double-check attached documents for accuracy and completeness.
Using a review and validation checklist can significantly reduce the likelihood of errors during submission.
How to Sign the Hospital Cash Claim Form
The Hospital Cash Claim Form requires a signature to validate the claim. Claimants may choose between digital signatures or traditional wet signatures. The eSigning process using pdfFiller is user-friendly and ensures compliance with all necessary regulations, making the process seamless and secure.
What Happens After You Submit the Hospital Cash Claim Form?
After submission, claimants can expect a systematic claims processing timeline. Typically, submissions are tracked, and claimants will receive confirmation once their forms are processed. For those needing to amend or check the status of their claims, it's advisable to maintain communication with GMS for updates and further instructions.
Enhance Your Experience with pdfFiller for the Hospital Cash Claim Form
Utilizing pdfFiller for the Hospital Cash Claim Form streamlines the filling process. Features such as 256-bit encryption and compliance with HIPAA and GDPR ensure that sensitive documents are handled securely. The platform also offers user-friendly tools to make editing and signing easy, providing a seamless experience for claimants.
How to fill out the Hospital Claim Form
-
1.Access the Hospital Cash Claim Form on pdfFiller by searching for its title in the pdfFiller document library.
-
2.Once you locate the form, click on it to open within the pdfFiller interface.
-
3.Before filling out the form, gather necessary information such as your personal details, illness or injury specifics, and physician information.
-
4.Begin filling in your personal information in the designated fields, ensuring to input accurate details like your name, address, and insurance policy number.
-
5.Use the checkboxes provided to indicate relevant options, ensuring clarity in your selections.
-
6.Input details about your illness or injury in the appropriate section, along with the dates of hospitalization or treatment.
-
7.In sections requiring physician information, fill in the name, contact details, and any other required specifics.
-
8.Review the entire form carefully before finalization to ensure all fields are correctly filled and all required information is included.
-
9.Once you’ve completed the form, utilize the review feature on pdfFiller to check for any errors or omissions.
-
10.After ensuring accuracy, save your work at any point using the 'Save' feature, and once complete, download a copy of your filled form.
-
11.Submit your form directly through pdfFiller if the option is available, or download and submit via email or postal mail to the insurer as instructed.

Who is eligible to use the Hospital Cash Claim Form?
The Hospital Cash Claim Form is intended for individuals covered under a group medical services insurance plan seeking to claim hospital cash benefits due to illness or injury.
What supporting documents are required with the claim form?
When submitting the Hospital Cash Claim Form, attach supporting documents such as discharge papers from the hospital and a physician's confirmation to validate your claim.
How can I submit the Hospital Cash Claim Form?
You can submit the Hospital Cash Claim Form by downloading a completed copy from pdfFiller and sending it via email or postal mail to your insurance provider, following their specific submission instructions.
What are common mistakes to avoid when filling out the form?
Common mistakes include leaving blank fields, incorrect personal details, failing to attach required documents, and not signing and dating the form before submission.
Is there a deadline for submitting the Hospital Cash Claim Form?
It’s crucial to check your specific insurance plan for any deadlines regarding claim submission, as they can vary, but timely submissions are generally advised to avoid claim denials.
How long does it take to process the claim after submission?
Processing times for claims can vary based on the insurer but typically range from a few days to several weeks. Check with your insurance provider for specific timelines.
Can someone else fill out the form on my behalf?
Yes, family members or designated representatives can complete the Hospital Cash Claim Form on behalf of the claimant, but a signature from the actual claimant is typically required.
Related Forms








Get the latest insights from our blog


If you believe that this page should be taken down, please follow our DMCA take down process
here
.
This form may include fields for payment information. Data entered in these fields is not covered by PCI DSS compliance.